Introduction
Reluctance to report research findings may arise from fear of retaliation from pharmaceutical or device corporations when findings are contrary to corporate interests.1,2 Research is increasingly funded by pharmaceutical corporations, which introduces bias toward publication of favorable results.3 We previously reported that actions taken by industry and academic leaders against clinicians who authored adverse drug reaction reports were mostly punitive.1,2 Case studies describe threats from pharmaceutical executives to clinicians when findings contrary to corporate interests were communicated. Attacks on scientists’ and clinicians’ character or their methodologies are threats described in case narratives, although no systematic review of threats and intimidation has been reported. In our study of fourteen clinicians who authored oncology-related serious adverse drug reaction reports, 83% experienced professional harms.1 In our study of eighteen clinicians who authored serious drug reaction reports for drugs with $1 billion or more in annual revenue, 61% experienced professional harms.2 Our objective is to expand upon case report literature and these two case series on harms to report on threats and intimidations targeted against clinicians and scientists who communicated, or attempted to communicate, findings contrary to corporate interests.
Methods
The principal investigator of a National Institutes of Health (NIH)-funded pharmacovigilance initiative established at the University of South Carolina (2011–2020) and at Northwestern University Feinberg School of Medicine (1998–2010) queried by email all clinicians or scientists at over fifty universities in the United States, Europe, Canada, and Asia who had previously served as first or last author of SONAR or RADAR peer-reviewed publications identifying important but previously unrecognized serious adverse drug reactions (SH, DMA, BD, TBH, BS, BJW, PSR, PRY, MLF, WJH, JMR, HST, JMM, MWS, KK, STR). These individuals were asked to identify instances where they personally presented findings contrary to corporate interests and subsequently experienced publicly documented threats from pharmaceutical manufacturers. These clinicians or scientists were asked to identify colleagues (clinicians or scientists) who had experienced similar publicly documented threats. Overall, twenty clinicians and six scientists included in this analysis had been publicly threatened or intimidated after communicating, or attempting to communicate, findings related to safety, efficacy, or data integrity between January 1, 1980, and December 31, 2020, and quoted in publicly available documents specifics of threatening activities (Table 1). Individuals identified as potential candidates for this study by RADAR/SONAR collaborators were excluded if public documentation of threats was unavailable. Using publicly available documents, information about motivations for conducting research with findings contrary to corporate interests and timing of related threats and intimidation was abstracted. Weekly, three research assistants who had independently abstracted the study data and two study senior investigators (CLB, SH) reviewed the abstracted data. Individual researchers reported on assessments of researcher motivation and reporting of threats, intimidation, and harms against clinicians or scientists of interest. Additional analyses provided information on time in months between threats and intimidation, harms, and regulatory notifications and also the magnitude of the costs incurred by patients, academic institutions, and pharmaceutical corporations. Qualitative analyses characterized scientists’ and clinicians’ primary motives for communicating their findings based on statements included in publicly available documents into the following categories: concerns related to patient safety, drug efficacy, or data integrity. This framework was developed with consultant input in our 2019 and 2021 studies on harms of reporting serious adverse drug reactions.1,2
Data
Data sources for threats included publicly available reports from government agencies, Congressional hearings, and an investigation commissioned by the Canadian Association of University Teachers, documents produced for jury trials and settlement agreements, Department of Justice press releases, and news articles primarily from The New York Times, The Wall Street Journal, The Guardian, The New Yorker, and Science. Data focused on information about manufacturers; clinician and scientist authors’ experiences of threats, intimidation, and harms; numbers of persons experiencing toxicities related to drugs or devices that were the focus of communications; payments for injuries/deaths associated with toxicities; and settlements or fines paid to government programs or affected patients. Interrater agreement was 98%, with one disagreement over whether the research had focused on patient safety or data integrity. The study’s principal investigator resolved this disagreement, supporting the data integrity focus. Safety-related drug/device withdrawals were identified from FDA’s public announcements. Additional information included publicly reported dates of FDA approval, communications of findings, details of publication, boxed warnings, and withdrawal of drugs or devices from marketing.
Analyses
Threats and intimidation were characterized according to concepts described in case reports as being against the “messenger” and/or against the “message.” For several individuals, threats and intimidations were followed by harms, including: loss of employment, job demotion, delayed academic tenure decisions, personal payments of legal fees for lawsuits filed against individual clinicians and scientists after public communication of clinical or basic science findings, loss of grant funding, and loss of academic positions.2 Formal documentation of corporate efforts to harm careers of clinicians or scientists were sought in materials obtained via discovery during court proceedings or as part of government- or university-commissioned investigations.
Clinicians’ and scientists’ stated summaries of personal experiences with the communication process were categorized according to whether the relevant employer was described as supportive, antagonistic, or neutral to communication efforts.
Median and ranges for time from FDA approval date to public reporting, receipt of perceived threats by clinicians or scientists, box warning addition, or drug/device withdrawal from marketing were calculated. Total criminal fines paid by corporations included in this study were also determined.
Role of the funding sources
The study sponsors had no involvement in study design, data collection, analysis, data interpretation, report writing, and the decision to submit.
Results
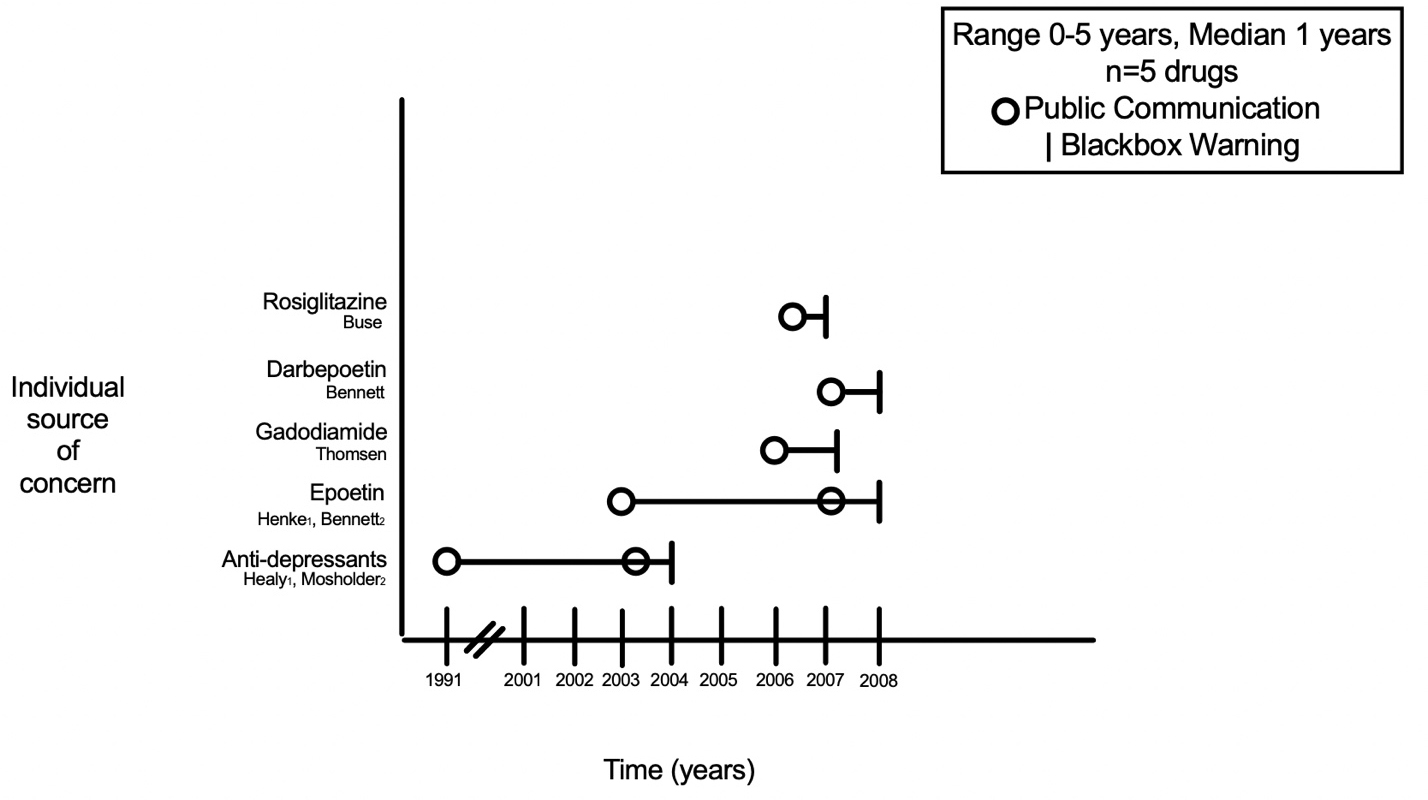
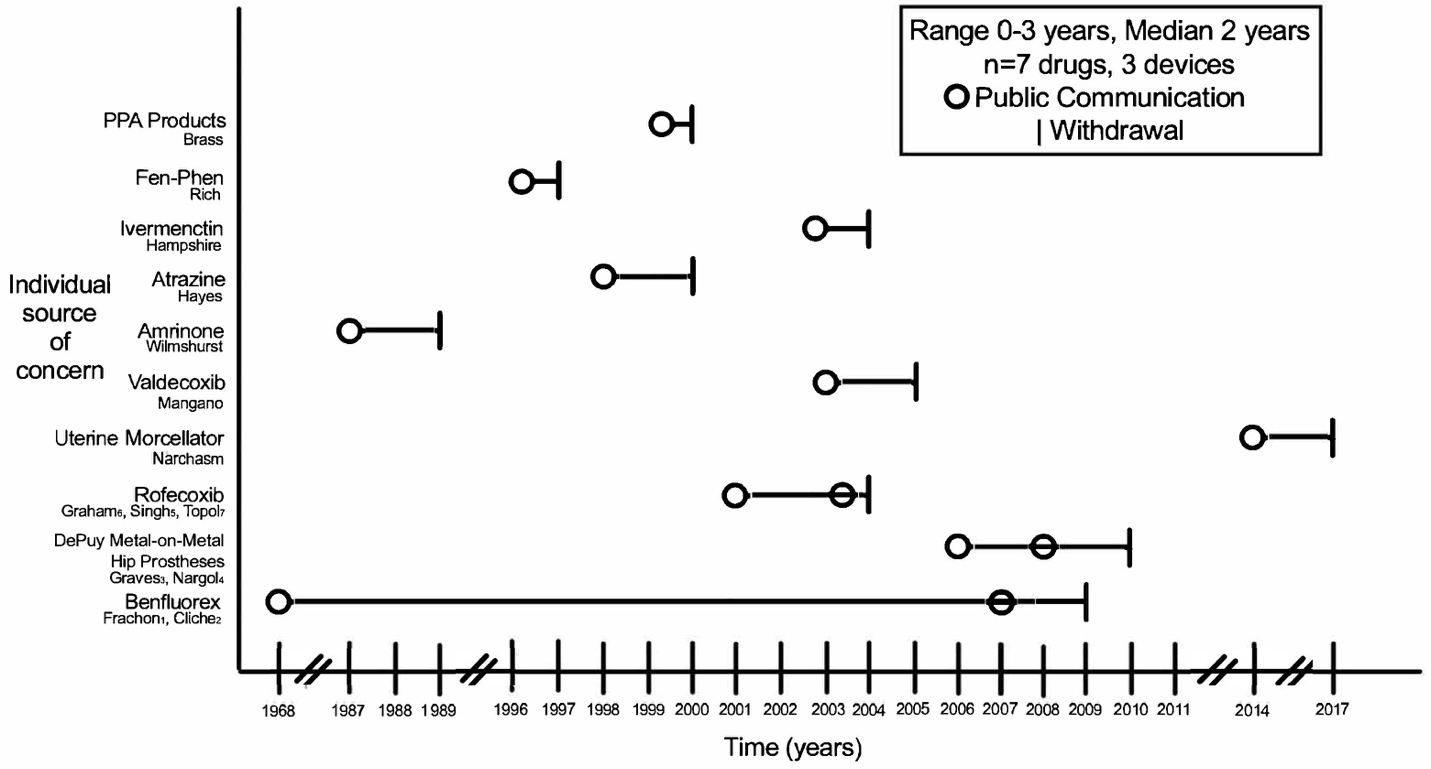
Multiple sources document clinicians’ and scientists’ findings of harm or lack of efficacy of pharmaceuticals and medical devices.10,14,21,24,43,47,55,62–71 These communications described toxicity or deaths,11,14,43,47,55,62–68 failure to identify efficacy,10,69–71 mechanism of action,21 and radiographic findings (Tables 1 and 2).24 A median of ten years separated dates of communications of findings and regulatory approval of relevant drugs or devices (range: zero years prior to fifty-eight years following FDA approval). A median of two years separated dates of initial communication to drug/device withdrawal or black box warning (Figures 1A and 1B).


Patient Impact
Of the twenty-six drugs and one device included in this study, twelve drugs and two devices were withdrawn from marketing, black box warnings were added to labels of six drugs, one device’s application for FDA approval was withdrawn, and one drug’s initially proposed submission of an FDA application for approval was delayed by thirteen years (Figures 1A and 1B). These responses occurred at a median of two years following initial scientist or clinician public communication efforts.
An estimated one million persons developed serious toxicities or died from adverse drug reactions from drugs and devices discussed in this article (Table 4). Fenfluramine-phentermine was implicated in serious injury or death in three hundred thousand persons.104 A related drug, benfluorex, was implicated in two thousand deaths.78 Ivermectin/pyrantel was associated with 552 reports of deaths occurring among dogs.105 Between 88,000 and 140,000 serious coronary heart disease events in Americans were estimated to have been caused by rofecoxib.42
Payments
Payments to patients and/or government agencies following investigations of sixteen adverse drug or device reactions exceeded $25 billion (Table 4). Median corporate settlements for civil, criminal, and shareholder lawsuits were $761 million (range: $3.6 million for benfluorex to $22 billion for fenfluramine-phentermine).50,106 Sales of four drugs decreased markedly following FDA meetings on toxicities of four drugs (epoetin and darbepoetin dropped from $7.1 billion collectively in 2007 down to $3 billion collectively in 2008),107 gadodiamide (dropped from $1 billion in 2006 down to < $100,000 by 2009),36 and rosiglitazone (dropped from $3 billion in 1999 down to $680 million in 2008).108 For fourteen additional drugs and one device (Figure 1B), sales decreased to zero following of removal of the product from the market.
Data sources
Nine communications were based on reviews of clinical trial data (Table 1). Five instances involved clinicians and scientists who were initially prevented from presenting their findings. One bone physician reported being unsuccessful in obtaining original phase III clinical trial data for an industry-sponsored trial in which he had conducted laboratory studies for the study popuation.21 A pharmacy professor reported being denied corporate permission to publish results of an industry-sponsored clinical trial in the Journal of the American Medical Association although she had designed the trial, had been the study’s principal investigator, and had received an acceptance letter from an editor at the journal.69 A radiologist reported being denied permission to report bone radiograph findings at a medical conference in Europe from a pharmaceutical company–sponsored phase III clinical trial that had been completed eight years previously and for which the study data had been stored at her academic institution.24 A hematologist confidentially reported to the Hospital for Sick Children’s Research Ethics Board that data from then unpublished phase II and phase III clinical trials identified lack of sustained effectiveness of the then-investigational iron chelating drug.20 She revised the consent forms, submitted revised forms to the Research Ethics Board, and these were approved. Four days later, the corporate sponsor prematurely terminated the clinical trials and issued threats of lawsuits. Study patients enrolled prior to the termination continued to receive the experimental drug under revised forms. Relevant safety data, with the hematologist as first author, were subsequently published in the New England Journal of Medicine.20 Lawsuits against the hematologist followed many threats issued by the corporate sponsor and were filed many years after the New England Journal publication. An epidemiologist reported identifying rofecoxib-associated cardiovascular toxicity following review of a phase III clinical trial study report.40 The epidemiologist, who is a senior investigator at the Food and Drug Administration, was informed by his superiors that he would not be allowed to present his findings at a medical conference in Europe. Subsequently, these findings were published a year later in an article that appeared in The Lancet.42
Five communications were from clinicians and scientists who were prevented from presenting findings of phase III clinical trial results. A radiation oncologist publicly reported and published findings in the Lancet of increased mortality rates with erythropoietin administration to cancer patients during an industry-sponsored phase III clinical trial.14
A gastroenterologist and a cardiologist independently and publicly reported cardiovascular toxicity with rofecoxib administration.4,9 An endocrinologist reported rosiglitazone-associated cardiovascular mortality after reviewing results of several phase III clinical trials.109
Case series were published by five clinicians describing patient safety concerns. One pulmonologist and one cardiologist reported pulmonary and cardiac safety concerns following short-term off-label use of a diabetes drug, benfluorex.63,64 A radiologist and a nephrologist reported chronic kidney disease patients who developed nephrogenic systemic fibrosis following magnetic resonance angiograms performed with a gadolinium-based contrast agent.65
Personal clinical observations informed toxicity reports from three clinicians. A surgeon reported development of metastatic sarcoma after his wife underwent uterine morcellation.68 One orthopedic surgeon in Australia reported that several of his patients had developed serious complications following DePuy metal-on-metal hip prostheses.52 A psychiatrist reported two patients had committed suicide after initiating anti-depressant therapy.93
Four case-control studies (one on phenylpropanolamine, two on anorectic drugs, and one on rofecoxib),43,47,64,106 two meta-analyses (one on erythropoiesis stimulating agents and one on anti-depressants),62,95 one review of FDA reports (on ivermectin pyrantel),53 and two basic science reports (one on frogs and one on corn)55,67 informed additional communications.
Five instances involved clinicians and scientists who were initially prevented from presenting their findings. An epidemiologist reported identifying rofecoxib-associated cardiovascular toxicity following review of a phase III clinical trial study report.40,106 The epidemiologist, who was also a senior investigator at the Food and Drug Administration, was informed by his superiors that he would not be allowed to present his findings at a medical conference in Europe. Subsequently, these findings were included in an article that appeared in The Lancet.42
Instances where scientists and clinicians identified fraudulent data submissions from pharmaceutical corporations
The communications identified seventeen individuals who identified eleven instances where corporate employees had submitted data to government or regulatory agencies that were subsequently identified as differing from source data belonging to clinician investigators of the same drug. These communications were related to two anorectic drugs (benfluorex and phenfluramine-fentermine), two cox-2 inhibitors (valdecoxib and rofecoxib), three devices (uterine morcellators, artificial hip implants, and a patent foramen ovale closure device), a cardiac drug (amrinone), a diabetes drug (rosiglitazone), anti-depressants, gadolinium-based contrast agents, an iron-chelating drug, a skeletal anti-resorptive agent, and a pesticide.6,9–11,18,21,30,33,34,40,42,43,55,56,63,65,68,70,71,87,109–114
Primary motivations for clinicians and scientists included concerns over drug/device safety (twenty-one individuals), drug/device efficacy (five individuals), or data integrity (one individual). Personal statements described negative interactions by tweny-three individuals with corporations, eleven individuals with university personnel, and four individuals with regulatory agency personnel.
Threats and Intimidation Efforts (Tables 1, 2, and 3)
Overall, twenty-three individuals received twenty-four threats from pharmaceutical employees generally within weeks of communicating concerns. Threats to fourteen individuals began shortly after presenting findings to pharmaceutical corporation employees. For ten individuals, threats began following presentations at medical conferences, or after being prevented by supervisors from presenting their concerns. Three individuals received threats from supervisors at regulatory agencies.
Intimidation efforts included: threats of lawsuits (eighteen individuals), public disparagement at conferences (eleven individuals), threats of loss of academic positions (six individuals), threats of loss of grant funding (two individuals), delays in decisions regarding tenure (two individuals), and threats of reassignment to a low-level position (one individual). Several documents identified complex efforts to intimidate scientists and clinicians.
5,12,20,22,25–27,31,34–37,51,53,54,56–61,75,82,92,110–113,115–136 Two clinicians incurred personal expenses over $1 million in attorney fees. One scientist described episodes where corporate scientists threatened his family.56 The Federal Office of Internal Affairs investigated an FDA reviewer after the reviewer’s account of selective serotonin reuptake inhibitors was forwarded to his supervisor.53 One clinician described receiving lawsuit threats after rejecting a financial offer by a pharmaceutical corporation to suppress publication of his findings.123 For twenty-three individuals, threats and intimidation efforts were sustained over long periods of time.
Threats and intimidation occurred for a median of three years (range: one to eighteen years). Some threats ended following regulatory actions. In two instances, threats were discontinued after executives for pharmaceutical corporations were contacted by academic department chairpersons.9,15 For two clinicians, threats persisted for more than a decade. Senior university and/or FDA officials took actions against twelve clinicians and four research scientists beginning a median of two years after the clinicians and scientists had publicly communicated their concerns (range: zero to five years).
Harms
For fifteen clinicians and scientists, threats were followed by harms. Harms were inflicted a median of one year after threats or intimidation began (range: zero to two years). Harms included personal payments of attorney fees (fifteen individuals), loss of hospital positions (nine individuals), loss of faculty positions (six individuals), loss of federal grants (two individuals), delayed tenure decisions (two individuals), removal as lead of a multi-national clinical trial (one individual), removal as a journal editorial board member (one individual), and job demotion (one individual). In fourteen cases, university employers provided support, overt or covert, to pharmaceutical companies against the clinicians and scientists. For three clinicians who lost university or hospital positions, their attorneys negotiated financial settlement agreements that also included non-disparagement clauses under which the clinician or scientist could not disparage the university. For twelve individuals, documentation of harms coordinated by a corporation was identified. In eleven instances, no university employee assisted a clinician or scientist. In one case, one clinician was awarded $39 million in damages and $19 million in interest from Pfizer and a statistician purportedly hired by Pfizer who had been charged with stealing data from the clinician’s laboratory. This data identified valdecoxib-associated cardiac toxicity.123 Before the case went to trial, Pfizer offered the clinician $24 million to settle.123 In 2009, a judge dismissed the verdict against Pfizer. The clinician reported that his attorney fees had been $15 million.123
Corporate-university interactions
Clinicians and scientists received threats from executives at eleven publicly traded corporations. These corporations ranged from smaller public corporations ($1.1 billion in market capitalization) to extremely large public corporations (market capitalization of $483 billion). Executives at two privately held companies also threatened three individuals. Twelve individuals who identified findings contrary to corporate interests were employed at eleven academic universities, each of which has more than 20,000 students. The University of California/Berkeley, the University of Toronto, the University of Sheffield, Northwestern University, and the University of North Carolina each had in-place or pending financial agreements with manufacturers who employed individuals who threatened eight scientists at the five universities.20,22,27,51,56,57,107,116–122,127,133 At Senate hearings, Drs. Buse, Singh, and Topol testified about communications from pharmaceutical executives to university officials requesting that these individuals be removed from their academic positions.5,9,15,142 Other examples of corporate-university interactions against scientists and clinicians involved Dr. Dong, at the University of California/San Francisco, Drs. Hayes and Chapala at the University of California/Berkeley, and Dr. Kern at Brown University, who were informed that their universities would not provide legal support against actions brought by pharmaceutical corporations.25,26,31,56,57,127,133,135
Criminal misdemeanors and fines against corporations (and one corporate executive)
Of the 13 pharmaceutical companies included in this report, four companies pled guilty or were found guilty in criminal trials (Table 4). The findings were related to six products (Table 4). Fines accounted for $5.7 billion in payments to the United States (for five products) and $3.3 million to the French government. The criminal pleadings were for misbranding, providing false information for commerce, failing to report clinical trial data, manslaughter, and causing patient deaths (Table 4).48,91,108,143–145 These guilty findings were related to pharmaceutical or device manufacturers knowingly reporting false data to regulatory agencies or marketing products that had known serious or fatal toxicities, while none related to misbranding.
Discussion
Our findings of threats and intimidation following communication attempts or actual communication of scientific findings contrary to corporate interests have not been described previously. In interpreting our findings, several factors should be considered.
Threats and intimidation were long-lasting and were first noted following public presentations. Careers of thirteen clinicians and two scientists were affected for years. Abraham and Davis note the significance of legal threats and explain that even if litigation threats are not converted to lawsuits, threats can impact when evidence becomes publicly known.150
We found that university employers actively discredited reputations of clinicians who had publicly communicated findings contrary to corporate interests. Our study extends the analysis of Rhodes and Stain who posited that scientific disagreements between academics and pharmaceutical corporations cause academic establishments to fear the loss of industry and grant dollars.151 A related consideration is that academic leaders are concerned that lawsuits might be filed by corporations if toxicities are reported by academic scientists. These concerns were borne out in our study.
Another concern was that after threats were made by corporations to fourteen clinicians and four scientists, regulatory agencies discovered that these corporations had submitted applications for regulatory approval or for documentation of governmental regulation requirements that included data that differed from source information in each of these clinicians’ or scientists’ files. Subsequent investigations found that, in most cases, the data submitted by the corporations was fraudulent.
In one of the most frequently cited reviews of a case involving disagreements between a senior clinician and pharmaceutical company in 1996, a pharmaceutical company prematurely discontinued two clinical trials led by Dr. Nancy Olivieri following generation of data potentially adverse to commercial interests and after attempting to discredit her.20 In 2009, an FDA review by the Division of Scientific Investigations of Olivieri’s clinical data from 1996 identified differences in data included in a 2009 sponsor’s application for FDA approval of deferiprone.152 A FDA site visit carried out in 2009 confirmed that, where source data were available from 1996, the 1996 data were accurate.
At the other end of the public awareness spectrum, in a serious but infrequently cited example of pharmaceutical fraud, the Netherlands Committee for the Evaluation of Medicines contacted Peter Wilmshurst in 1983 about discrepancies between published toxicities with amrinone and amrinone toxicities reported by the sponsor. Comparison with original reports of phase III clinical trial data revealed that the sponsor had altered case report findings.11 The pharmaceutical sponsor attempted to discredit Dr. Wilmshurst before prematurely discontinuing a phase III clinical trial with amrinone.
Following threats and intimidation of clinicians and scientists, regulatory agencies delayed taking safety-related actions that would have positively affected public health (Figures 1A and 1B). The priority of profits over people resulted in delays of several years for withdrawals or black box warnings for most drugs and devices reported herein.
Fourteen clinicians or scientists experienced personal harms. Harms ranged from loss of professional positions (nine individuals) to payments of attorney fees of $1 million (two individuals) and $15 million (one individual). A distinguishing characteristic between the fourteen individuals who experienced harms versus the twelve individuals who experienced threats and intimidation but no harms was that individuals who experienced harms had generally been disciplined by university or regulatory authority employers after publicly communicating findings contrary to corporate interests.
The circumstances involving disciplinary actions against six clinicians and three scientists were reviewed extensively by committees or external reviewers. In each case, detailed investigations concluded that the university or a regulatory agency had purposefully intimidated and threatened the clinicians and scientists and the clinicians and scientists had not been at fault. It should be noted that following disciplinary actions taken by four universities or medical centers against four individuals, the university or hospital paid financial settlements to these four individuals. Three settlements required the clinician to sign non-disparagement clauses (only the financial settlement involving Healy did not). Only one university-convened committee reported that a clinician’s personal action supported a disciplinary decision. The University of Sheffield had disciplined a radiologist for submitting an abstract to a medical conference without receiving permission to submit the abstract to the conference. Following this action, the clinician was dismissed from the university. Grant funded research was a major component of the academic careers of five clinicians. Only one of these five clinicians continued with an active grant-funded research career.
Our study included individuals who reported threats or intimidation. Roy Poses, editor of the well-respected blog Health Care Renewal, described in detail intimidation efforts involving five clinicians.116,117,120 He concluded: “I am convinced that for every Aubrey Blumsohn, there are dozens who are aware of deception, other unethical conduct, even crime and corruption that could harm patients and patient care, but are afraid to speak out.”116 Moreover, though several SONAR/RADAR investigators and collaborators published clinical findings contrary to corporate interests, no documented threats or intimidation acts could be identified after the findings were published.153–162
Our study has limitations. There might be whistle-blowers who have been publicly threatened by corporations and were not identified by our search methodology. However, our findings suggest that based on the search criteria that we developed, the likelihood of having missed many of these scientists or clinicians is small. Our estimate of $25 billion in financial settlements/payments and one million injuries or fatalities represents significant damage. If individuals were omitted from our search, then the financial and human cost estimates might be much larger (i.e. the “tip of the iceberg”).
There are additional data about each case that were not identified in our searches. These data include sealed judicial documents and undisclosed financial settlements, findings of university investigations that are not publicly disclosed, an in-press report (i.e. a review of the Bennett-Amgen and Bennett-Northwestern University cases by Jack Getman JD, emeritus Earl E Sheffield Regents Professor of Law at the University of Texas and former general counsel to the American Association of University Professors),163 and secrecy clauses between universities and/or corporations and scientists or clinicians that prevented dissemination of additional information.29,103,120,129,135 Also, while some of the claimed threats and harms (e.g. harms such as loss of grant funding, loss of position) could be spurious, this is unlikely. Clinicians and scientists in this study testified under oath at Congressional hearings, had corroboration of individual claims in an external report from professors at other universities (for Chapela), a report from the Canadian Association of University teachers (for Olivieri), an in-press report on the Amgen-Northwestern University case (for Bennett), and as part of presentations made when receiving an honorary doctorate or an award from the American Academy of Advancement of Science (for Oliveri) or after receiving excellence awards from various honorary societies and organizations (for Wilmshurst and Hampshire).20,29,53,54,127,128,133,135,164
It should be noted that these twenty-six individuals differ from the usual description of qui tam relators (“whistleblowers”) who file fraud claims involving federal funds, are frequently characterized as disgruntled employees, and, if successful, receive significant financial remuneration for their efforts. None of the twenty-six individuals received any financial remuneration for communicating findings contrary to corporate interests. Several clinicians and scientists faced libel lawsuits after reporting their findings.12,35,36,136,140
To our knowledge, this is the first case series reviewing threats and intimidations experienced by clinicians and scientists who identified significant findings contrary to corporate interests. Our results indicate that while commitment to accurately reporting findings related to patient safety, drug efficacy, or data integrity was the most common motivating factor for twenty-six individuals, clinicians and scientists should be aware that extended threats or intimidation efforts can occur after these communications are publicly disseminated. Schafer and Krimsky summarized approaches to mitigate effects of pharmaceutical and academic threats when reporting findings potentially contrary to corporate interests.130,165 The first option, termed the regulatory approach, focuses on managing risks that accompany pharmaceutical funding. The second approach eliminates corporate sponsorship of academic research. These approaches could have assisted some individuals in this study who received direct manufacturer funding but would not have helped others.
Our study suggests that corporations (and pharmaceutical employees, if their role is known) who knowingly submit fraudulent data to support regulatory agency requirements for drugs or devices should be tried for criminal violations. There is some precedent for this. In 2021, former Servier Incorporated executive Jean-Philippe Seta received a four-year suspended sentence in a case that involved thousands of patient deaths and severe injury to tens of thousands of patients.146 Between 2009 and 2021, four of the thirteen corporations accounting for six drugs or devices and included in this study pled guilty to varying criminal charges (Table 4).48,91,108,143–145 Going forward, more criminal activities conducted by pharmaceutical or device corporations are likely to be uncovered, as in the case of Purdue Pharma. As in the Servier executive case, focused efforts are needed to hold corporate executives accountable. The many examples of threats and intimidation that resulted from medical researchers exposing corporate wrongdoing discussed in this paper show that corporate executives must be held responsible for these actions.
Data Sharing Agreement
All data were obtained from publicly available data sources as cited in the methods, tables, and references. Each co-author had full access to the entire study database.
Guarantor
Charles L Bennett MD PhD MPP is the guarantor of the accuracy of this manuscript.
Acknowledgments
We are particularly indebted to the long series of conversations and guidance on this project from the late Robert C. Kane MD, the 2016 Frances Kelsey Award Recipient from the Food and Drug Administration who died in 2018 before completion of this manuscript. We would like to thank clinicians and pharmacovigilance experts who have worked closely with the National Institutes of Health–funded R01 grants, the Southern Network on Adverse Reactions (SONAR), and the Research on Adverse Drug Events and Reports (RADAR) projects at: the University of South Carolina, Columbia, South Carolina; the Medical University of South Carolina, Charleston, South Carolina; Duke University, Durham, North Carolina, University of North Carolina, Chapel Hill North Carolina, Tulane University, and the Louisiana State University, New Orleans, Louisiana, the University of Miami, the University of Texas, San Antonio, Texas; the University of New Mexico, Albuquerque, New Mexico; Nara Medical University, Kashihira, Nara, Japan; the Japan Institute of Pharmacovigilance, Tennoji-ku, Osaka, Japan, the MD Anderson Cancer Center, Houston, Texas; Johns Hopkins University, Baltimore, Maryland; the University of Nebraska School of Medicine, Omaha, Nebraska; Baylor University, Houston, Texas; the University of Chicago, Chicago, Illinois; the University of Illinois/Chicago, Chicago, Illinois; Indiana University, Indianapolis, Indiana; Case Western Reserve University, Cleveland, Ohio; Albert Einstein College of Medicine, Bronx, New York; the Mission Saint Joseph’s Hospital, Asheville, North Carolina; University of Copenhagen, Copenhagen, Denmark; Yale University, New Haven, Connecticut; University College, London, England; University of Modena and Regio Emilia, Modena, Italy; the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institutes of Health, Bethesda, Maryland; the Food and Drug Administration; Silver Spring, Maryland; the University of Copenhagen, Copenhagen, Denmark; McGill University, Montreal, Canada; the University of Pennsylvania, Philadelphia, Pennsylvania; Rutgers University, Piscataway, New Jersey; Washington University, Saint Louis, Missouri; Memorial Sloan Kettering Cancer Center, New York, New York; the Midwest Center for Health Services Research and Policy Studies, Maywood, Illinois; Tenon Hospital and Pierre and Marie Curie University, Paris France; Singapore General Hospital, Singapore; Hotel-Dieu, Paris, France; Queen’s University, Kingston, Ontario; the University of California at Los Angeles, Los Angeles, California; A Manzoni Hospital, Lecco, Italy; the University of Utah, Salt Lake City, Utah; Oregon Health Sciences University, Portland, Oregon; the Therapeutics Good Administration, Cabrera, Australia; Long Island Jewish Medical Center, New Hyde Park, New York; the Veterans Administration Cooperative Studies Program Clinical Research Pharmacy, Albuquerque, New Mexico; University of Pisa, Pisa, Italy; Stanford University, Palo Alto, California; the University of Pisa, Pisa, Italy; the University of Melbourne, East Melbourne, Australia; the Dana Farber Cancer Institute, Boston, Massachusetts; the Neoplastic and Autoimmune Diseases Research Institute, Rancho Santa Fe, New Mexico; the Southern Illinois College of Medicine, Springfield, Illinois. The names of the individual investigators are not included to protect the confidentiality and anonymity of collaborators of RADAR and SONAR. We acknowledge helpful comments from Aubrey Blumsohn MD, Peter Wilmshurst MD, David Healy MD, David Kern MD, and Terence Young. We acknowledge helpful comments on the conceptualization of the project from Eric Topol MD, Stephen Nissen MD, Aaron Kesselheim MD JD, Karen Starko MD, and Michelle Mello JD PhD. We acknowledge uncompensated editorial support from Virginia Green PhD of the Benaroya Research Institute in Seattle, Washington, and Elizabeth Saenger PhD.
Declaration of interests
All authors have no financial or personal relationships to disclose.