
Introduction
Asbestos-related diseases (ARD), i.e. asbestosis, asbestos-related changes of the pleura, asbestos-related lung, larynx or ovarian cancer and malignant mesothelioma have gained particular importance as occupational diseases worldwide.
The diagnosis of ARD is based on a detailed personal interview of the patient, occupational data on asbestos exposure in the work history, pulmonary physiology and radiological findings, i.e., results of chest X-ray and, if necessary and available, high-resolution chest computed tomography.1 For compensation according to the German occupational disease no. 4104 (Berufskrankheitenverordnung, BKV)2,3 malignant tumors such as lung cancer, larynx cancer, ovarian cancer or mesothelioma have to be confirmed by histopathological examination. The diagnosis of asbestosis and asbestos-related pleural changes can be made if radiological findings correspond to a work history compatible with significant asbestos exposure.4
However, the exposure to asbestos fibre dust from previous decades in the workplaces cannot always be adequately reconstructed due to lack of fibre measurements and/or incomplete information in work biographies. An alternative attempt was therefore made to correlate the asbestos fibre and/or asbestos body concentrations in the lung tissue with potentially ARD to estimate past occupational asbestos exposure in general5–7 or amphibole asbestos exposure in particular.4
With limitations (see Discussion section below), such analyses of lung tissue for asbestos fibres and FB may provide data to supplement occupational history.
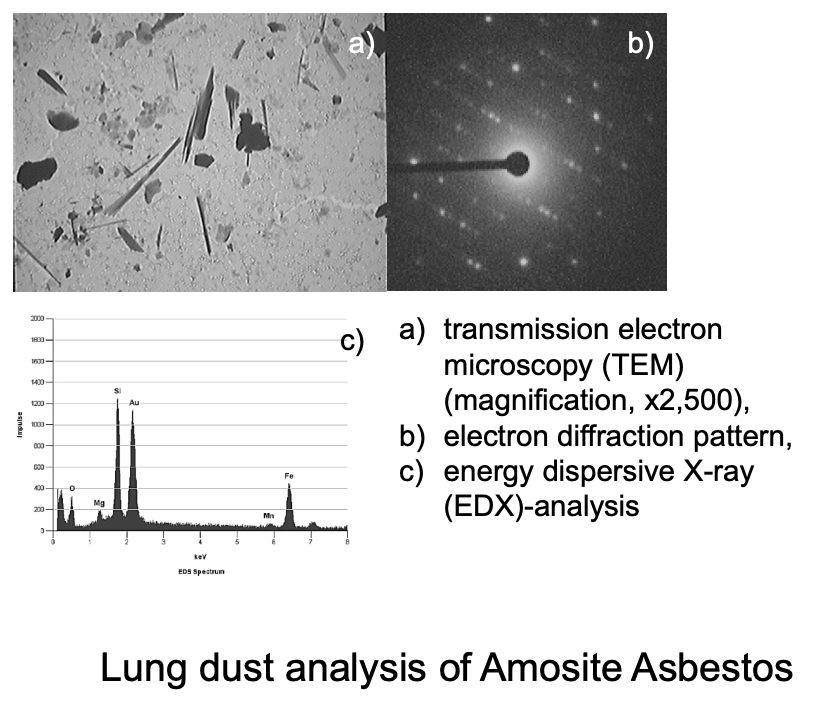
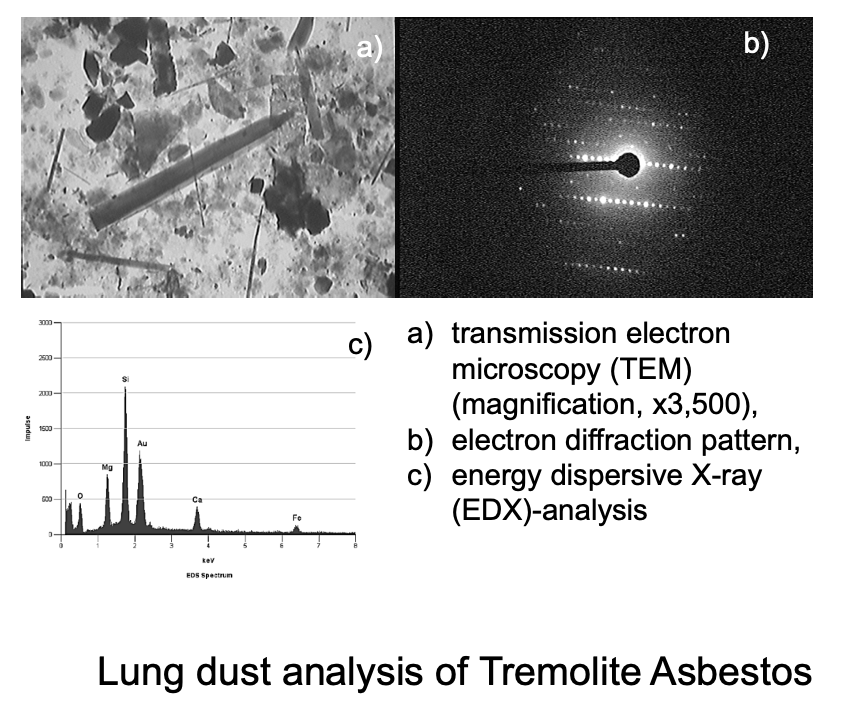
With regard to analytical methods, scanning electron microscopy (SEM) identifies fibre geometry in addition to the microstructure of the fibres. Energy dispersive X-ray spectroscopy (EDX) determines elementary composition. The crystallinity of fibres was additionally investigated with transmission electron microscopy (TEM) and electron diffraction. Using this method, it is possible to identify the different types of asbestos fibres as well as other mineral fibres. For clinical purposes, ferruginous (asbestos) bodies (FB) can be counted in lung tissue specimen as well as in ashed lung using light microscopy (Leitz Diaplan, Wetzlar, Germany) by use of 500x magnification.
Manke et al.8 evaluated the application of a plasma ashing method for STEM fibre analysis in human lung tissue. In order to carry out a complete check of the preparation method, a suspension of standard crocidolite fibres was used. No changes in length, diameter or aspect ratio distribution occurred during low temperature ashing method. Up to 78% of the fibres were recovered.
Asbestos and other inorganic mineral fibres in human lung tissue analyzed by an analytical scanning transmission electron microscopic method (STEM) at the Institute and Outpatient clinic for Occupational and Social Medicine at the University of Giessen in Germany, headed by Prof. Woitowitz, showed that the correlation between the estimated cumulative workplace exposure in fibre-years and the biomonitoring of asbestos content in the lungs is weak.9,10 This is caused by chrysotile asbestos – around 95% of asbestos used in Germany and also in many other countries – which is not biopersistent in the lungs and rarely form FB.9,11 Scanning electron microscopy (SEM) (Hitachi S-2300) was used with magnification up to 100,000. This allows to detect particles until 20 nm diameter. Chrysotile asbestos fibres can splice lengthwise. All fibres of a length > 5 µm were counted, also fibres with extremely small diameters (BIA_Arbeitsmappe). Crocidolite asbestos fibres were counted when they meet the WHO fibre criteria (WHO fibre definition of length (L) > 5 µm, diameter (D) < 3 µm, ratio of length to diameter (L/D) >3:1). These fibres have been thought to be especially relevant for carcinogenicity and fibrogenicity. In addition to fibres of L > 5 µm fibres of all length (L>1 µm) can also be taken into account; for instance broken crocidolite fibres. Fibres between 1 and 5 µm length were detected and analysed separately in the last 20 years. Scanning electron microscopy (SEM; Hitachi S-2700; Hitachi, Ltd., Tokyo, Japan) was used to identify particle geometry in addition to the microstructure of the fibers. The element analysis resulted from energy dispersive X-rays (EDX). Transmission electron microscopy analysis combined with electron diffraction (detection of crystallinity) was performed using a transmission electron microscope (H-7100; Hitachi, Ltd.).
Given the German asbestos ban in 1993, the question arises as to whether and what concentrations of asbestos fibres can still be detected in the human lung tissue after an interim period of more than 20 years. In this study, we quantified lung asbestos fibre and FB counts as well as cumulative exposure data from medical expert opinion procedures (fibre-years) in patients with ARD. We did not aim to reevaluate the histopathology diagnosis of the study group.
Material and Methods
Since 1982 lung dust fibre analyzes have been carried out by the Institute and the Outpatient Clinic for Occupational and Social Medicine. 257 such lung dust fibre analyses were done in potentially asbestos-related occupational diseases for diagnostic medical expert opinions on behalf of German social courts and statutory accident insurance institutions. The German diseases definition which combines asbestosis and asbestos-related pleural disorders. An in-depth occupational history was taken from all patients examined by experts and a standardized cumulative asbestos dose estimate was carried out based on the BK report’s “fibre-years”.12 Detailed clinical investigations according to the guidelines on diagnosis and compensation of ARD,1 combined with the occupational history data, had shown that 28 patients suffered from asbestosis as diagnosed by case history indicating asbestos exposure, computed tomography and/or chest X-ray, lung function testing. 105 suffered from primary lung cancer (59.2 ± 10.0 years) and 44 from diffuse malignant pleural mesothelioma (59.8 ± 10.0 years). 46 were controls without previous asbestos exposure undergoing lung surgery due to lung cancer associated with smoking, emphysema bullae or suspected hypersensitivity pneumonitis, and 34 other controls not exposed to asbestos had diseases not involving the lungs.
Methodological details (including sampling, operating materials and accessories, preparation, counting of ferruginous bodies and asbestos fibres, suspension and resuspension, calibration, documentation and calculation of the results, detection limits, influences on measurements and measuring uncertainty, classification of fibres and their documentation, quality control measurements, calculation of mean values, interpretation of findings, European inter-laboratory test results etc.) are described in the BIA-Arbeitsmappe13 which was developed in cooperation with our working group at the University in Giessen, Germany. In brief, approximately 2 cm3 of the formalin-fixed lung tissue obtained surgically or post mortem was cut into 3-5 mm pieces and mixed. About half of the material was freeze-dried for electron microscopy. A wet/dry factor (mean value 10) was determined from the ratio of the wet and dry weights to convert the concentrations from g/wet to g/dry (gdry) lung tissue. The light microscopic preparation for counting FB was obtained from the other half of the tissue using a modified NaClO method.10
When the starting material was paraffin blocks from the histological preparation of the patient’s lungs, the lung tissue was excised from the block and completely deparaffinized by heat treatment and subsequent washing in xylene.
Further sample preparation included plasma ashing of the tissue and subsequent quantitative filtration of the remaining lung ash. Transmission preparations were made from the filter for SEM (Hitachi S-2300; Hitachi, Ltd., Tokyo, Japan) and TEM was used to identify fibre geometry in addition to the microstructure of the fibres. To determine the elemental composition Energy Dispersive X-ray spectroscopy (EDX) was applied. The crystallinity of fibres was additionally investigated with transmission electron microscopy (TEM) and selected area electron diffraction (SAED). To increase the conductivity, all samples were sputtered with a fine layer of Au.
Fibre counting was done at 10,000x magnification in grid fields with an area of 0.01 mm². The searched area is up to 0.25 mm² for fibres of all lengths and up to 0.5 mm² for fibres with a length ≥ 5 µm. The lower limit of fibre detection is determined by the blank obtained with an empty filter impinged with aqua bidest; it can also result from the sensitivity of the analytical method, i.e. from the fibre concentration found on an impinged filter as well as on the effort and time of counting [VDI 3492].14 From the number of fibers on the filter and by use of Poisson statistics the lower limit of detection is calculated from For fibres with a length of ≥ 5 µm the lower limit of detection is 0.02 fibres/gdry lung tissue. According to the VDI 3492 the lower limit of detection can be defined as the concentration of three identified fibres (i.e., the three-fold of the sensitivity). The mean sensitivity is about 28,000 fibres/gdry lung tissue. The mean fibre concentration of about 20,000 is mentioned instead the upper 90 percentile with 40,000 fibres, because many detection limits are even below 10,000. For statistical calculations the use of numbers is necessary. No detection of asbestos fibres is not the same as “missing value.”
Tremolite asbestos has not been used commercially in Germany but minimal contaminants by tremolite in some asbestos products cannot be excluded.
The correlation between the asbestos fibres observed in the lung dust fibre analysis using STEM and the FB concentrations were calculated with SPSS 20.0 according to Spearman’s rank correlation test.
In the following section, the asbestos fibre or FB concentrations per gram of dry lung tissue (FB/gdry) are presented.
To illustrate, with a section thickness of a histological preparation of 5 μm, a tissue cube with an edge length of 1x1x1 cm would result in 2000 histological sections. The detection of an asbestos body in the section corresponds to a concentration of 2,000 FB per cm3 of lung tissue.
Results
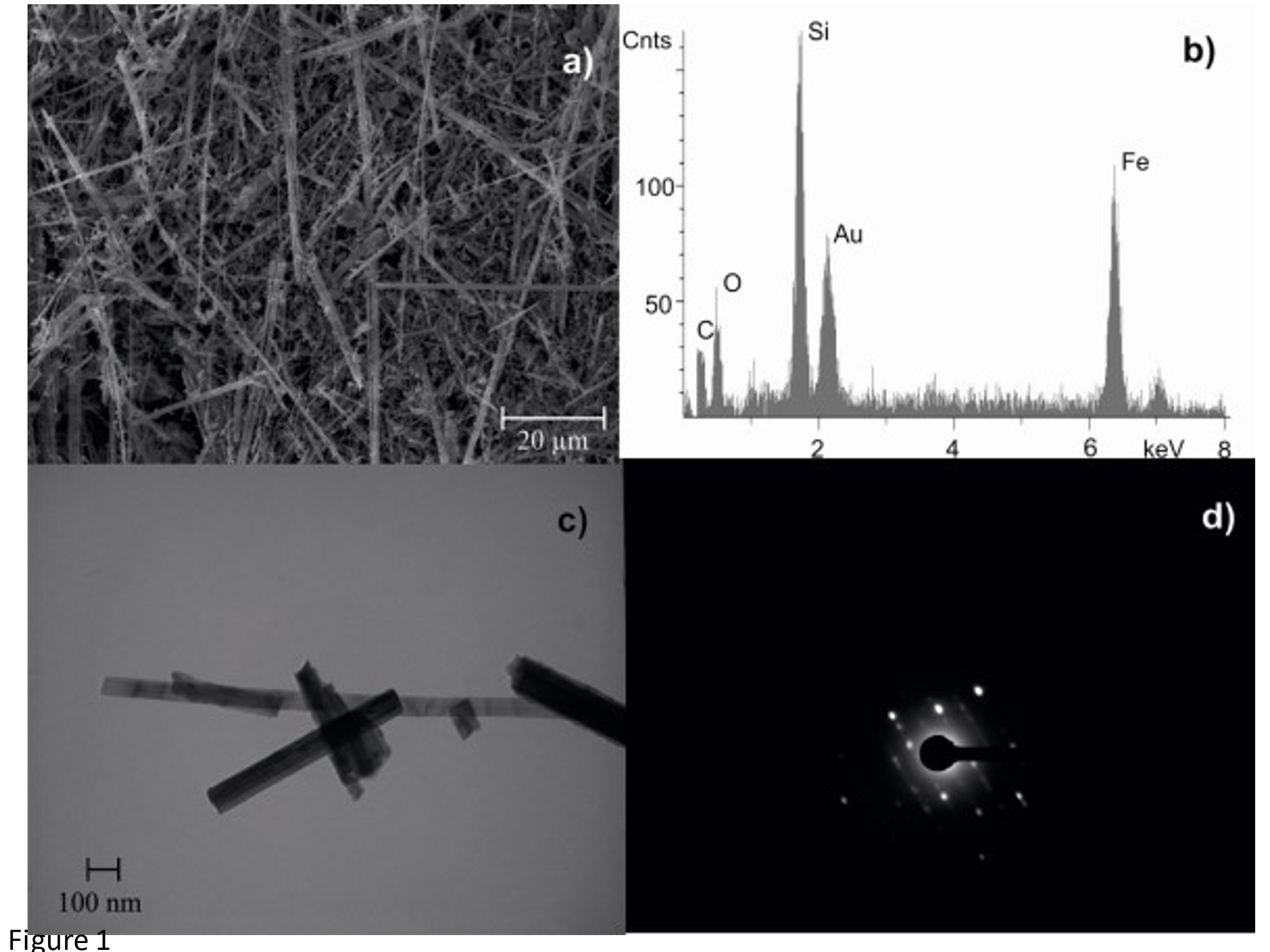
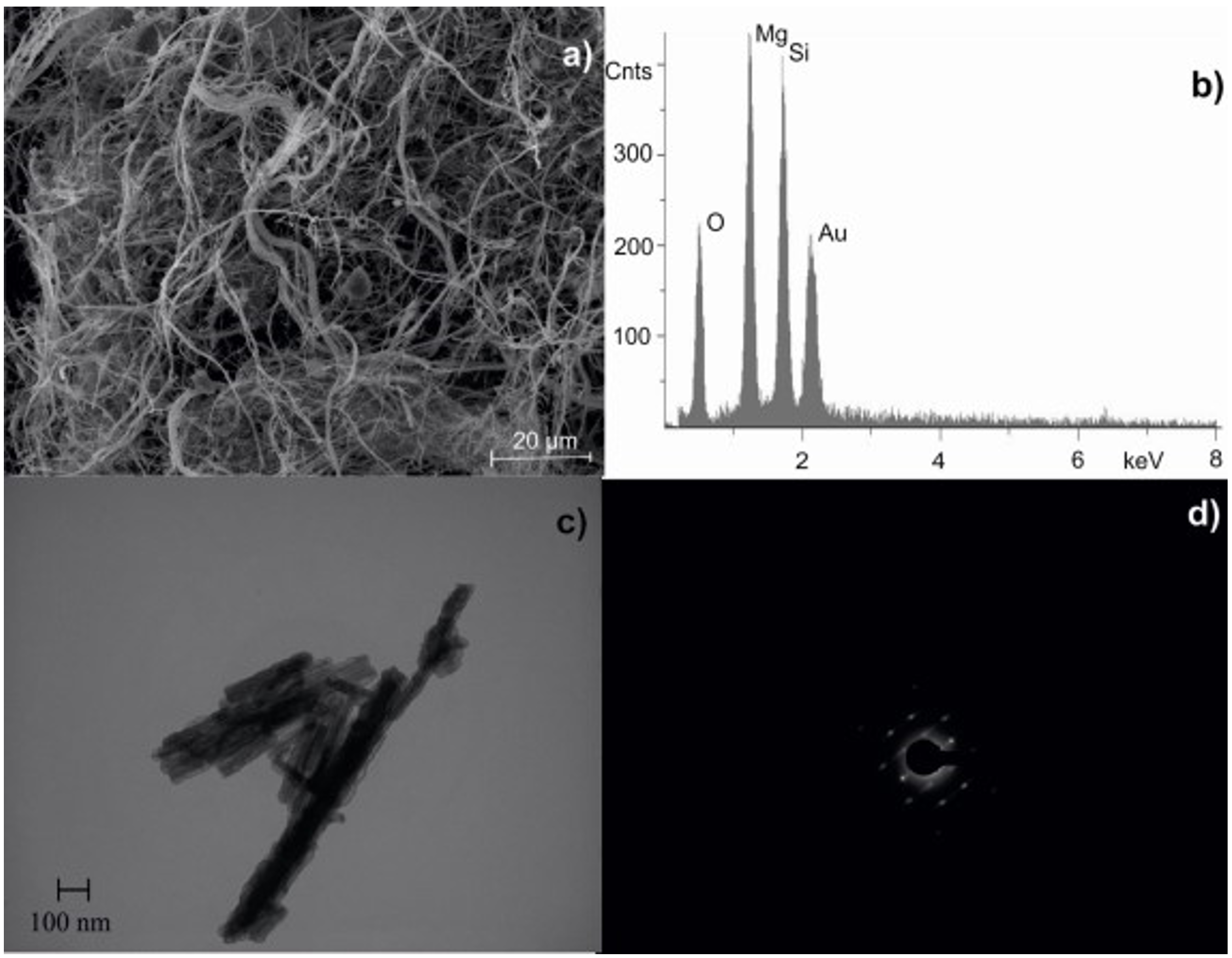
In a previous study of our institute asbestos fibres were identified as follows: 28 % chrysotile asbestos, 4 % amosite asbestos, 4 % anthophyllite asbestos and 68 % crocidolite asbestos.15 Figures 1 and 2 represent characterization of UICC crocidolite and chrysotile fibres.


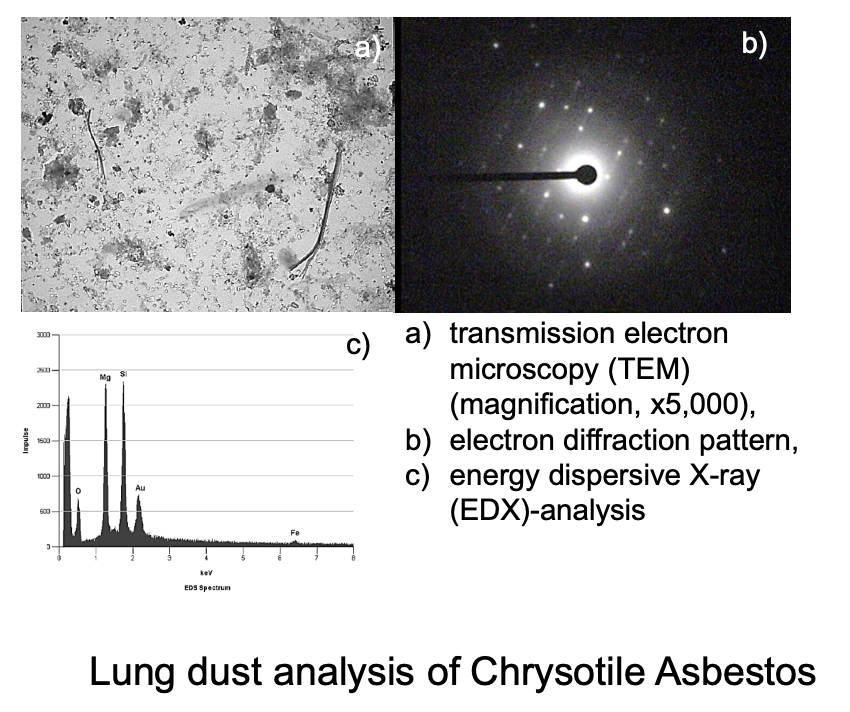
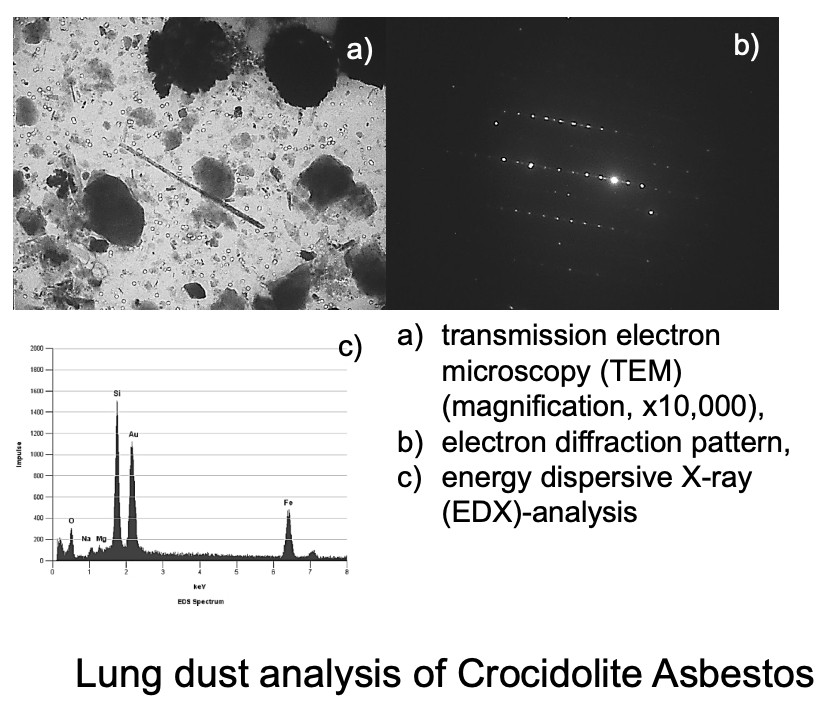
Figures 3 a, b, c, d show individual asbestos fibre types identified in lung dust analyses of this study. The fibre type shown in Figure 3 d was rarely found in lung tissue; the Fe peak may also represent some actinolite fibres which cannot be separated from tremolite.




Chrysotile and amphibole fibre concentrations as well as FB counts in the lung tissue are roughly associated with the cumulative asbestos exposure levels in the workplace. Fibre concentrations were found to be independent of the disease. On average, about 50,000 chrysotile fibres/gdry were found with asbestos dust exposure below 20 fibre-years, and about 190,000 chrysotile fibres/gdry with asbestos dust exposure above 20 fibre-years. The corresponding concentrations were 300,000 and 9,200,000 F/gdry for amphibole asbestos and 12,000 and 41,000 FB/gdry for FB. The difference between the groups with high or low asbestos exposure was significant for chrysotile asbestos (p = 0.011), and crocidolite asbestos (p = 0.004), and FB (p = 0.021).
In the lungs of 17 control subjects without any history of asbestos exposure (so-called “normal population”), upper limits of 180,000 fibres F/gdry with a length > 5 μm for chrysotile fibres and 140,000 F/gdry for amphibole fibres (length > 5 μm) were determined; 78 FB per cm3/ g dried lung tissue were counted in controls.
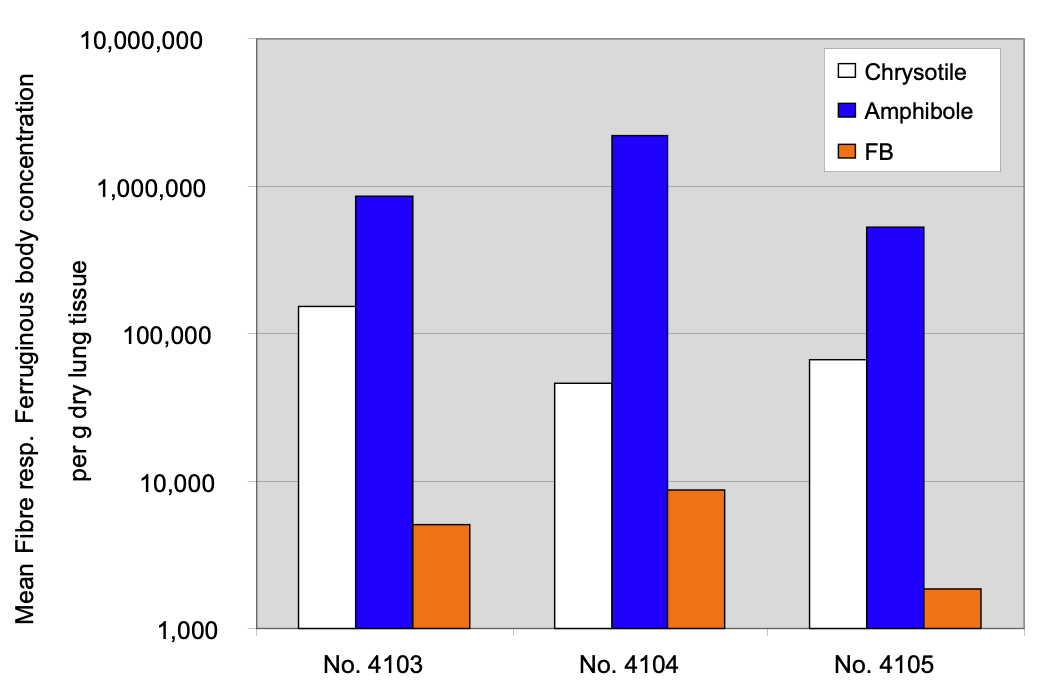
According to the diagnoses “asbestosis and/or asbestos-related pleural changes”, “asbestos-related lung cancer” or “diffuse malignant mesothelioma”, a large range of fibre concentrations were measured without any significant differences between these asbestos-related diseases (Fig.4). Mean chrysotile fibre concentrations were 152,000 in patients suffering from asbestosis, 46,000 in those with lung cancer, and 67,000 F/gdry in patients with mesothelioma. Mean amphibole fibre concentrations were 850,000 in patients with asbestosis, 2,200,000 in lung cancer cases, and 532,000 F/gdry in patients with mesothelioma. Mean FB concentrations were 5,100 FB/gdry in patients with asbestosis, 8,800 FB/gdry in those with lung cancer, and 1,840 FB/gdry in those with mesothelioma.

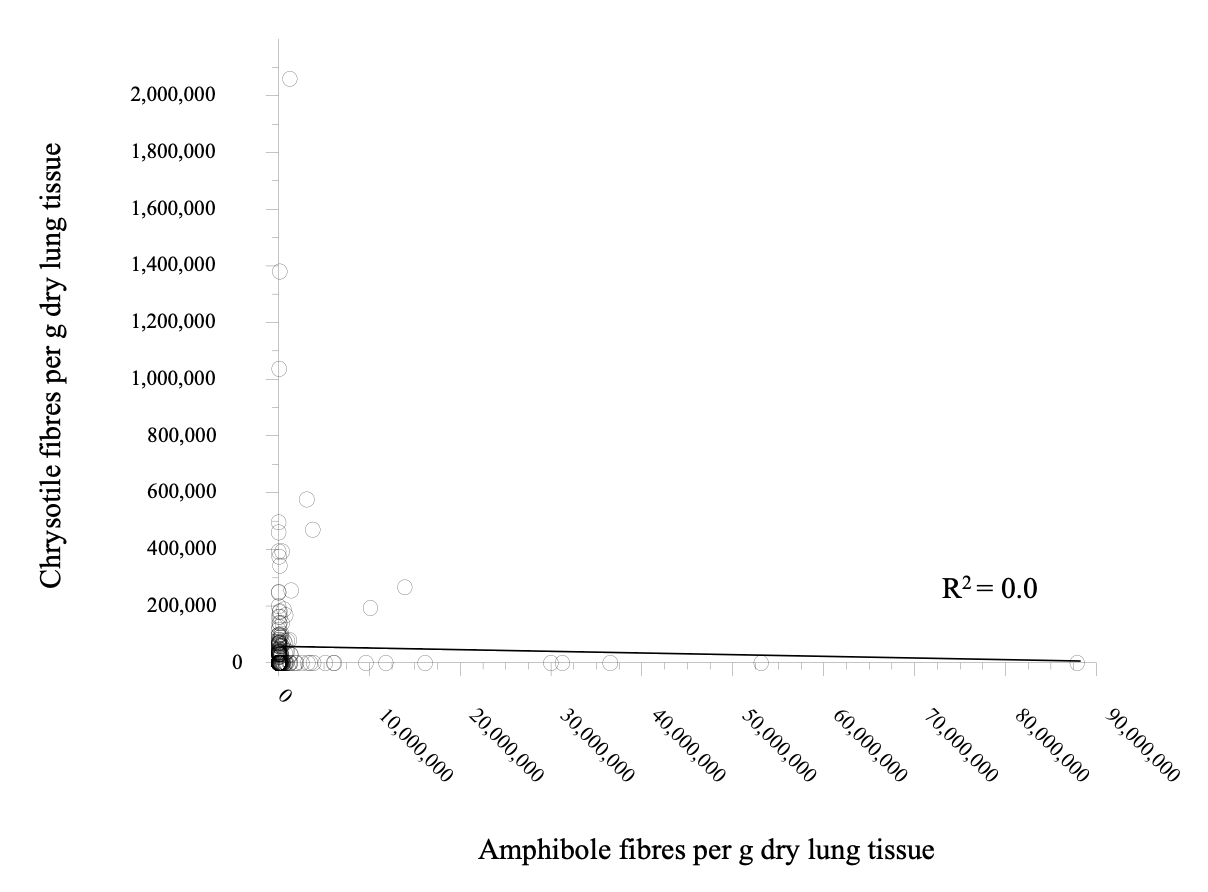
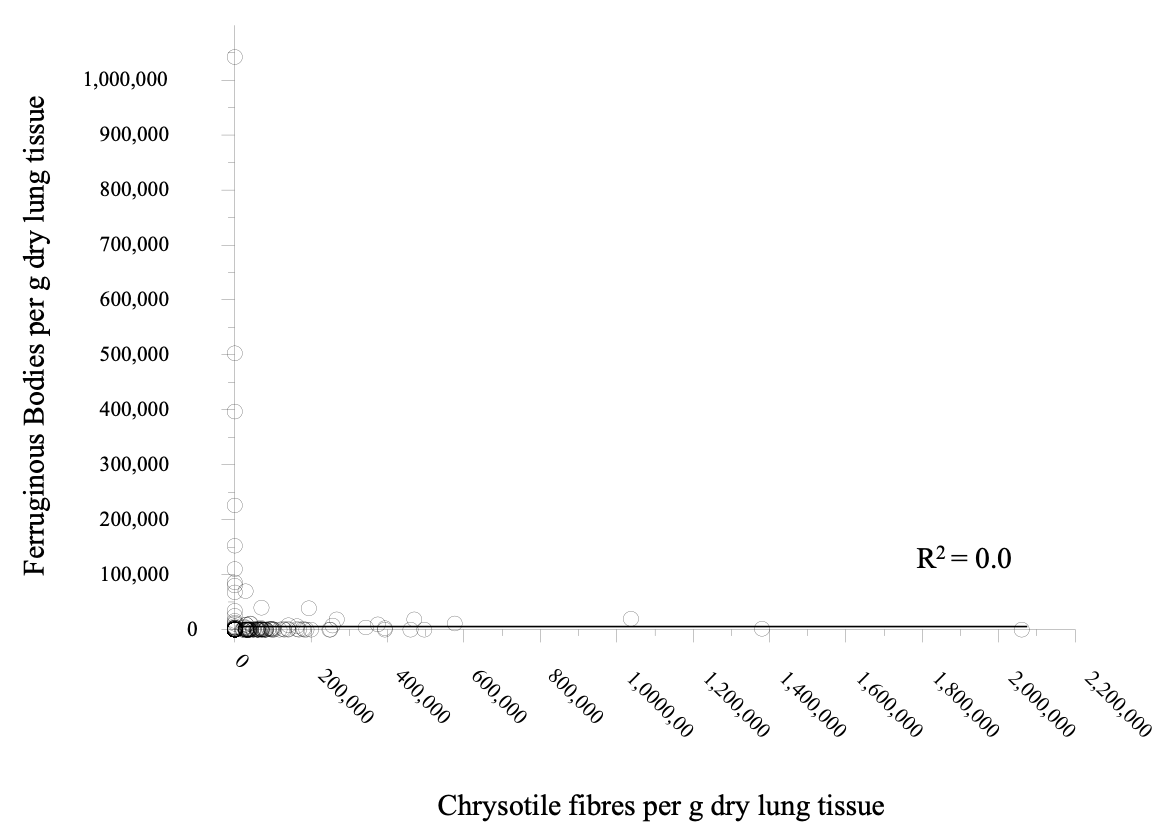
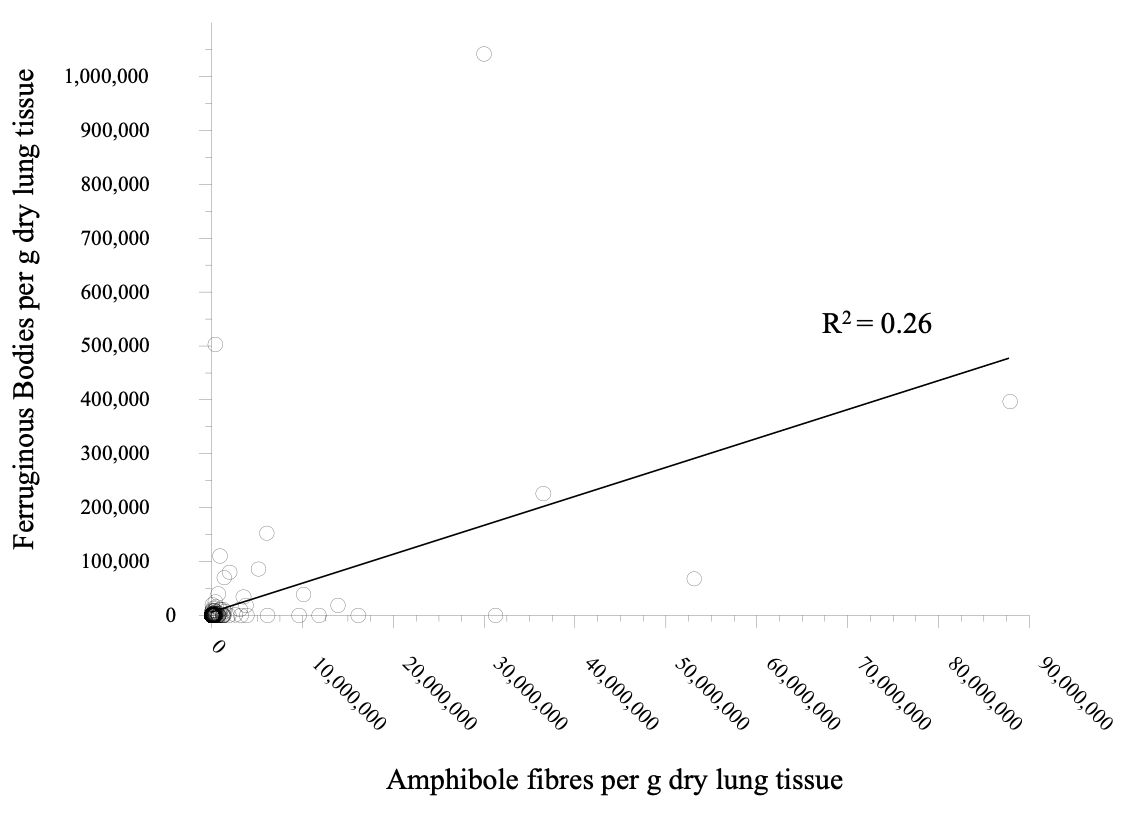
For asbestos fibres with a length > 5 μm determined in the lung tissue using STEM and the FB concentrations per gram of dry lung tissue, there was neither a correlation between chrysotile and amphibole asbestos fibre concentrations (Fig. 5) nor between chrysotile fibre and FB concentrations (R2 = 0.0) (Fig. 6). There was a weak correlation (R2 = 0.26) between amphibole fibre and FB concentrations (Fig. 7), which is obviously due to the known longer biopersistence and the higher FB rate of amphibole fibres compared to chrysotile fibres.



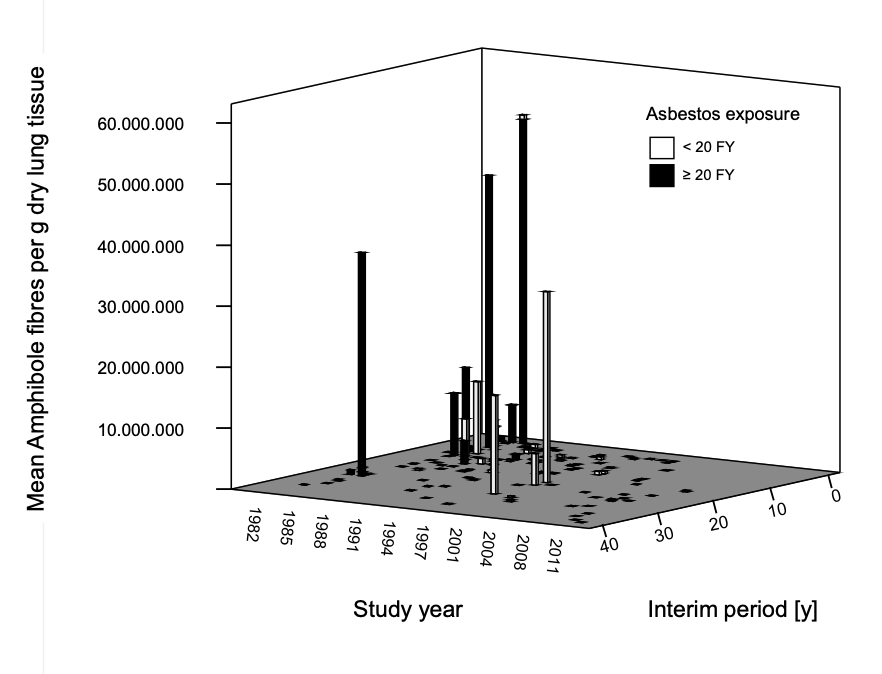
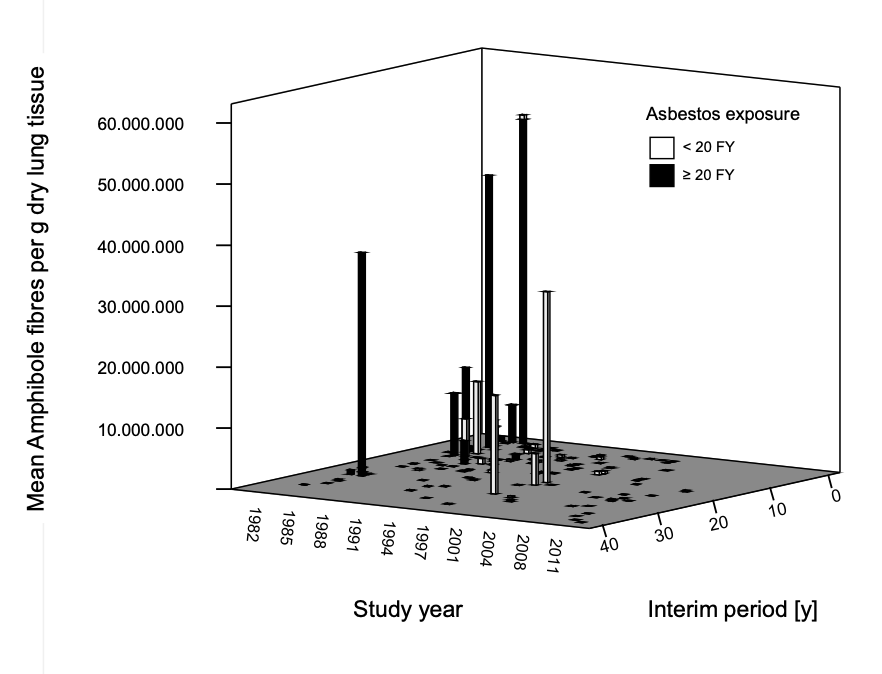
The asbestos fibre concentrations depended in particular on the time lung tissues was taken and the interim period. The highest asbestos fibre concentrations and FB were measured in the 1980s for interim periods of less than 1 year but decreased significantly with increasing interim periods (Figs. 8-10). After an interim period of more than 20 years, hardly any chrysotile or amphibole fibres were detectable. The overwhelming majority were other mineral fibres (for instance man-made mineral fibers, refractory ceramic fibres, talcum, gypsum). After the year 2000, i.e. 7 years after the German asbestos ban and decreasing asbestos levels in the worksites over the 3 decades before,16,17 it was only possible to detect occasionally asbestos fibres in the lung tissues.



Discussion
Asbestos fibres are mostly resilient in the environment. However, they undergo elimination kinetics in the lungs. In the lung environment, chrysotile fibres leach magnesium and fan out into fibrils with a diameter in the range of 0.02 – 0.2 µm.18 Chrysotile fibres are rapidly cleared, especially those short in length are transferred to the pleura, peritoneum, and pericardium. Suzuki et al. found 30 times more chrysotile than amphibole fibres in mesothelial tissue.19 Such fibres were also detected in neighboring organs.20–27 Low biopersistence of chrysotile in lung tissue has been demonstrated by various authors in animal experiments and in previously exposed workers.19,24,28–32 Bernstein et al.33,34 report half-lives of only a few days in rats; however, these experiments have been criticized for significant bias in the pretreatment of the fibres and the failure to take account of fibre translocation to the pleura and to neighboring organs.35,36 In animal studies it was shown that the clearance half-life of Canadian chrysotile asbestos depends on the fibre length and is mostly in the range of days, but half-life of long chrysotile fibres in human lung was shown to be several years. Corresponding findings were reported in Quebec miners undergoing autopsy.37
Accordingly, Churg wrote:
“The available data suggest that chrysotile is deposited in the parenchyma but is cleared extremely rapidly, with the vast bulk of fibres removed from human lungs within weeks to months after inhalation; by comparison, amphibole clearance half-lives are of the order of years to decades”.
Churg and Wright 199430 added
“…although some fibres may be sequestered and very slowly cleared. Overall, these studies suggest that the differences between amphibole and chrysotile fibre burdens in man reflect much faster clearance of chrysotile fibres, rather than a failure of chrysotile deposition”.38
Similarly, Neumann, Theile et al. formulated "Thus chrysotile is removed from the lungs very quickly".39
Everatt et al. were able to detect chrysotile in the lung tissue in only 18 of 302 cases (298 lung cancer, 4 mesothelioma) of whom 22.2 % had a cumulative asbestos dose of at least 5 fibre-years.40 Friedrichs, Dykers and Otto examined an employee who had worked in a (chrysotile) asbestos spinning mill for 5 years and after an interim period of 60 years they could identify chrysotile in only 10.3% of the lung fibres.41 Churg and dePaoli found
“..that the failure of chrysotile to accumulate in human lungs reflects events that occur early after exposure rather than long-term clearance mechanisms”,
noting no significant difference in chrysotile content after interim periods of less than 2 and greater than 12 years.42
Short fibres do not undergo ferruginous coating. There exist interindividual variation of ferruginous coating of long asbestos fibres with a subgroup of proficient “coaters”.
As opposed to chrysotile, amphibole asbestos types were shown to be much more biopersistent in the lungs, with half-lives of several decades.43,44
In accordance with the literature, our STEM lung dust fibre analysis shows that there was no correlation between chrysotile asbestos fibres and amphibole asbestos fibre concentrations each with lengths > 5 μm (Fig. 5) nor was there a correlation between fibre and FB concentrations for chrysotile asbestos (R2 = 0.0) (Fig. 6). Because of the longer biopersistence of amphibole asbestos fibres than of chrysotile asbestos fibres, and the predominance of short chrysotile fibres in the workplace long amphibole asbestos fibres in particular are converted to FB. Thus, there is some correlation between amphibole asbestos fibre and FB concentrations with a correlation coefficient of R2 = 0.26 (Fig. 7).
Chrysotile fibre, amphibole fibre, and FB concentrations in the lung tissue depend only roughly on the cumulative asbestos exposure levels in the workplace.9–11
For amphibole asbestos, the elimination kinetic in human lung is slower than that of chrysotile.
Furthermore, in our investigations no significant differences could be found between the lung asbestos fibre concentrations and the type of the asbestos disease, such as asbestosis/asbestos-related pleural lesions, asbestos-related lung cancer or mesothelioma; there was always a large range of the measured fibre concentrations (Fig. 4).
Correspondingly, the CAP/NIOSH definition of asbestosis does not consider quantification of asbestos fibres or FB for diagnostic purpose.45 However the CAP/NIOSH definition published more than 40 years ago was based on findings while asbestos exposure was high in many workplaces does not seem to represent the situation after introduction of an asbestos ban in the past, i.e. after a long interim period. There may be extensive lung fibrosis but since no ferruginous bodies, even with large amount of short chrysotile in lung tissue present, the pathologist may not attribute the fibrosis to asbestos or call the pathological observation by term asbestosis. If there is a biopsy or autopsy, no attempt to support or refute the history of exposure using lung fibre burden analysis should be done. We recommend to re-evaluate the CAP/NIOSH asbestosis definition in light of these findings and present workplace situations.
We recommend to re-evaluate the CAP/NIOSH asbestosis definition in light of present workplace situations.
With regard to fibre analysis, counting FB by light microscopy can only detect fibres with a diameter of up to 0.2 µm, and only fibres with a diameter of more than 1 µm can be classified on the bases of their optical properties.46 It is therefore not possible to detect and identify thin chrysotile fibres using a light microscope. In contrast, elementary fibrils of chrysotile can be identified with the analytical scanning transmission electron microscope (STEM). In our institute, Rödelsperger et al. coordinating a multi-center study found a total of 438 chrysotile fibres of all lengths and 163 chrysotile fibres with a length greater than 5 µm in a STEM lung dust analysis of 66 mesothelioma patients47; in controls not exposed to asbestos, respective figures were 812 chrysotile fibres of all lengths and 374 chrysotile fibres with a length greater than 5 µm. The definition of the so-called WHO asbestos fibres (length ≥ 5 µm, diameter < 3 µm; ratio of length to diameter greater than 3:1) is methodically determined. It aims to identify the carcinogenicity of long and thin fibres.48
Furthermore, previous transmission electron investigations of 134 FB from deceased patients who were predominantly exposed to chrysotile fibre dust in the workplace showed that only about 2.2% of them were attributable to chrysotile, almost 89.5% to amphibole, and 8.2% to other mineral fibres.47 From this it can be concluded that chrysotile hardly forms any FB, and therefore their measurement is only useful for histopathological diagnostics when FB can be detected. As a result, the proportion of histopathologically diagnosed asbestosis grade 1 (“minimal asbestosis cases”), which has been primarily based on the detection of FB, is very low in workers previously exposed to chrysotile. In the Mesothelioma Register in Bochum was a proportion of about 6-10% of asbestosis grade 1 within about 1,000 examined cases per year reported.6 Obviously, the real asbestosis figure is much higher, when generally accepted less restrictive diagnostic definitions45,49 would be applied. It has to be mentioned that the Mesothelioma Register has applied the non-substantiated restrictive asbestosis definition of Roggli et al.46 combined with the requirement of FB in the neighbourhood of fibrotic areas and a concentration of 2 AF/cm2 (Feder et al.5,6) (for details see below). There were severe criticism to this diagnostic practice which is not based on scientific data.50–52
It has to be mentioned that our work is limited insofar as patients’ numbers of subgroups with different ages, diagnoses and interim periods were too small for statistical analyses and we only considered fibres with a length of > 5 µm. Fibre counts in pleural tissues are not customary. Nevertheless, our data shows that the asbestos fibre content in human lungs depends only roughly on the cumulative exposure in the workplace, i.e. the duration and intensity of exposure, whereas its dependency on the interim periods is obvious. This means that hardly any generally applicable diagnostic data on asbestos fibres in human lung can be expected; this is especially due to the facts that
-
there is no worldwide asbestos ban and interim periods are therefore heterogenous,
-
in different countries various amphibole types - which, in contrast to chrysotile asbestos, are more biopersistent and lead to the formation of FB in a significantly higher proportion - were also used,
-
fibres are heterogeneously distributed in the lungs; so, individual probes may not be representative,
-
applied methodology of fibre analysis varies considerably and many associated analytical problems still exist,53,54
-
there exists only a limited number of respective qualified studies,
-
the fibrogenic and carcinogenic properties of short asbestos fibres (<5 µm) have only rarely been analyzed.8 Only a few publications report fibres of all lengths (greater than 1 µm), while many publications only report concentrations of WHO fibres with a length ≥ 5 µm. However, short fibres with a length of 1 to 5 µm also have adverse health effects. There is strong evidence that these short fibres are also carcinogenic and especially cause pulmonary fibrosis.22,55–58
All of the aforementioned facts demonstrate that from the diagnostic point of view the lung asbestos fibre and FB content in lung tissue is of very limited value. They indicate that a long past exposure to asbestos can usually no longer be confirmed by lung fibre analysis. This means in practice that a negative light or electron microscopic lung fibre analysis cannot overturn a qualified occupational history. The latter combined with a detailed industrial hygienist recording of occupational exposure remains the cornerstone of the diagnosis of asbestos-related occupational diseases.59
The aforementioned limitations of lung fibre counting are also relevant for pathohistological diagnostics. They imply that when diagnostic considerations are limited to counting FB (which mostly disregards chrysotile exposure) and to the long WHO fibres (≥ 5 µm in length), methodological problems arise in that chrysotile exposure, and exposure to short asbestos fibres in general, which obviously also cause pulmonary fibrosis and are carcinogenic,60,61 are not properly considered.
Pathohistological definitions of asbestosis are based on the detection of FB, although FB have no causal significance for asbestosis and other ARD, their numbers decrease with the interim period, and they are hardly reproducible and not generally applicable. If positive, they are merely an indicator that asbestos exposure has taken place. The pathohistological CAP/NIOSH definition of asbestosis grades 1 - 4, which is still favored by leading pathologists49 and also recommended by the American Thoracic Society (ATS),62 was developed by a large group of experts, subjected to a thorough, transparent review process and eventually received NIOSH approval.49 In contrast, the modified definition by Roggli et al. requires that in asbestosis grade 1 (so-called “minimal asbestosis”) the fibrosis affects not only the bronchiolus wall but also the first layer of adjacent alveoli.46 At the same time, for the normal finding (asbestosis grade 0), the determination according to CAP/NIOSH ("no fibrosis of the bronchioles") is converted by Roggli et al. into: "no significant peribronchiolar fibrosis, fibrosis limited to the bronchioles". This means that early asbestos-related changes, which are assigned to asbestosis grade 1 according to CAP/NIOSH, are classified as “normal” without scientifically proven justification.
In addition to the aforementioned histopathologically defined asbestosis grading by CAP/NIOSH, the definition of asbestosis by Roggli et al. additionally presupposes the detection of asbestos fibres in the fibrosis area and a minimum concentration of an average of 2 FB per cm2 of lung tissue. This average value according to Roggli et al. is not consistent with the experience of other leading pathologists.49,59,63–65 As mentioned, CAP/NIOSH does not require a minimum concentration of asbestos fibres or FB; only the histopathological findings of asbestosis and an association of individual FB with fibrosis are required.45
The CAP/NIOSH definition states: "Presently, the minimal features that permit the diagnosis are the demonstration of discrete foci of fibrosis in the walls of respiratory bronchioles associated with accumulations of asbestos bodies…. When only a single asbestos body is found in a histologic section, it is necessary to demonstrate additional asbestos bodies (either in deeper sections of the same block or in other sections of the same block or in other samples of tissue) to establish the diagnosis of asbestosis". It must be taken into account that, as explained above, under the current conditions in Germany and correspondingly in other countries with asbestos bans enforced decades ago there is generally no longer any evidence of an increased concentration of FB and asbestos fibres in the lungs of previous asbestos workers.
Roggli had recommended the aforementioned modified CAP/NIOSH system in the Helsinki criteria in 1997 and 2014.66–68 In 1997, the board of directors of the German Society for Pathology essentially followed this definition of minimal asbestosis69: "The internationally valid definition of minimal asbestosis (asbestosis grade I according to the Anglo-American nomenclature) includes the light microscopic evidence of minimal foci of fibrosis in the area of the bronchioli respiratorii and the accompanying vessels with maximum radiation into the directly adjacent alveolar septa and asbestos bodies stored in these areas. The random (one-off) detection of asbestos bodies is not sufficient to diagnose minimal asbestosis. A dust analysis limit value for minimal asbestosis has not been defined".69 Remarkably, this text also mentions the involvement of accompanying vessels, which is neither mentioned in the Roggli publication nor in the Helsinki criteria, without citing a specific source or original data.
The pathologists Hammar and Abraham state with regard to the aforementioned discrepant diagnostic criteria of Roggli et al.: “As a historical note, the criterion of the 1982 CAP/NIOSH criteria45 for requiring “more than one” asbestos body to be found in a single lung tissue section was based on the exclusion of the “chance” finding of a single asbestos body in the lungs of the general background population in which one asbestos body might be expected to be found in approximately 50–100 or more lung tissue sections of average area and thickness (each with a volume of approx. 10-3 cm3)”.49 Furthermore, these pathologists state: “If one considers that this recommended concentration of 2 asbestos bodies/cm2 of lung tissue section corresponds to approximately 4,000 asbestos bodies per cm3 or 4,000 asbestos bodies per gram of wet lung, one sees that this is at least 200 times higher than the upper limit of background asbestos body concentrations (20 asbestos bodies per gram of wet lung) relied upon by Roggli”.70
Conclusions
This work is limited insofar as the number of subjects in subgroups are too small for statistical analyses. Only numbers of WHO fibres (L > 5 µm, D < 3 µm, ratio of length to diameter (L/D) >3:1) were reported because these fibres have been thought to be especially relevant for carcinogenicity and fibrogenicity.
Our results demonstrate a clear decrease in identified chrysotile and amphibole concentrations as well as in FB in human lung tissue with increasing interim period. After an interim period of about 30 years, elevated chrysotile asbestos fibre concentrations cannot be detected in the lung tissue of formerly chrysotile-exposed workers. Also, as we could show for the first time, the more biologically stable amphibole asbestos fibres, such as crocidolite, are subject to elimination kinetics in the lungs. Therefore, false-negative results of lung dust fibre analysis must be expected not only for chrysotile asbestos, but also for crocidolite asbestos. This means that a negative light or electron microscopic lung dust analysis is not capable of overturning a reliable occupational history of asbestos exposure.32,71 Only in cases of questionable exposure to asbestos dust in the workplace or the environment lung dust fibre analyses may provide - in case of a detectable elevated fibre concentration - a supplementary exposure evidence.
Although historic histopathological definitions have required the detection of asbestos fibres and/or FB, nowadays these requirements which are based on findings at times with high asbestos exposures and a short or absent interim period, are of very limited diagnostic significance for ARD. We suggest a reevaluation of the CAP/NIOSH asbestosis definition for the current situation in many Western countries with asbestos bans and the consideration of exposure to predominant short chrysotile fibres. This is even more relevant for the more restrictive and not scientifically based diagnostic recommendations including the detection of FB or increased asbestos fibre concentrations in lungs as published46 and also introduced in the Helsinki Reports66–68 under the chair of the pathologist V. Roggli.72
Post scriptum: After submitting this manuscript for publication we noticed a new publication by Roggli et al.73 By analysing fibres of a length of 5 µm or more in 619 malignant mesothelioma cases the authors describe a strong decrease of elevated lung asbestos content from 90.5% in the 1980s to 54.1% in the 2010s (p < 0.001). Our data presented above are in line with this degree of the lung fibre load over recent decades. This supports our finding of fibre elimination depending on the interim period. However, the degree in the study of Roggli et al. is smaller than in our investigation which may be due to higher asbestos exposures with a still missing ban in the USA. There is strong evidence that the authors misinterpret their findings when concluding that an increasing percentage of malignant mesothelioma is not related to asbestos. A related wrong statement, namely that an increasing percentage of malignant mesothelioma is not related to asbestos, was repeatedly made by Roggli et al. when interpreting selected epidemiological data and ignoring environmental and household asbestos exposures.74
Disclosure statement
The authors declare that no competing interests exist.
Two of the authors have testified in occupational diseases litigation on behalf of plaintiffs, provide independent expert opinion for social courts or statutory insurances.
Funding
No funding supported this work.
Ethics approval
Ethics approval is not applicable.
Acknowledgements
The authors thank Mrs. Natalia Haibel, graduate engineer, for her technical support during the fibres analysis.
Parts of this manuscript were already published in German in a national journal, namely in “Zentralblatt für Arbeitsmedizin".1,2
-
Baur X., Schneider J. Validität faseranalytischer Verfahren in der Diagnostik asbestbedingter Berufskrankheiten. Zbl Arbeitsmed. 2021;71:128-143.
-
Schneider J, Arhelger R, Brueckel B. Lungenstaubanalysen in der Begutachtung asbestverursachter Erkrankungen. Zbl Arbeitsmed. 2015;65:305-309.
Copyright for use of the translated figures and some translated text was provided by the publisher (Springer).