
I. Introduction
In the United States, but less so in other countries, clinical and well-documented investigations on asbestos-related health risks have been published since the 1920s.1–4 It is now accepted that in most industrialized countries asbestos is the leading cause of work-related deaths. The global estimate of asbestos-related deaths is some 250,000 annually and for the twenty-eight member states of the European Union the respective figure is in the range of 100,000.5 Numerically, lung cancer resulting from work-related asbestos hazards is always near the top of the list6–10; one in every two to three deaths from occupational cancer is estimated to be caused by asbestos.7,11 This is also true for Germany with its previously (until 1989) separated parts of East and West. Currently there is a beginning decline of asbestos-related diseases with a mean latency of about forty years following the asbestos ban Germany legislated in 1993.12 In spite of the extensive ongoing WHO’s campaign to eliminate asbestos-related diseases (ARD) worldwide,7,11 only about 70 countries put a ban of asbestos in force; on the other hand, more than 140 countries have continued to allow asbestos to be used (most notably the USA).13
This paper is based on historical reflections, especially those of the first author, who was involved in early studies on asbestos exposure and related diseases in Germany, as well as in the regulatory processes associated with long-lasting opposition of industry corporates. To date the impacts of serious and decades-long breaches of vital health and safety regulations on asbestos have not been properly assessed and no one has been held accountable. In this context, the main objective of this article is to provide a review of corporate refusal to acknowledge asbestos-related adverse health effects and to pay substantiated compensation claims to asbestos victims.
II. Background
In 1871, Louis Wertheim in Frankfurt was the first German asbestos factory to start the production of asbestos goods utilizing imported Canadian chrysotile. For decades, the Dresden area has been home to one of the German asbestos industry’s oldest production facilities, the Saxony Asbestos Factory in Radebeul, which opened in 1878. During the Nazi period, i.e. from the late 1930s until 1945, asbestos became a broadly used strategic material, especially in the construction, textile, machinery industries.14 (see also volumes 7 and 8 of the Nurenberg trial.15,16
After World War II, asbestos-containing products accounted for the vast majority of roofing, wall cladding, and flooring, and were used for fire protection or as lightweight binding materials. An estimated 800 million to 1.3 billion square meters of corrugated and cladding panels containing asbestos cement were installed on roofs and on house walls by the construction industry. Almost three quarters of all Canadian chrysotile imports into Germany were used to manufacture these products.17 The wide range of different asbestos cement binding materials were ideally suited to the post-war reconstruction required at that time.
These asbestos cement products were used and applied at countless construction sites which resulted in extremely high asbestos exposures for many occupational groups, especially those in the building trades. Roofers, façade and ventilation builders, and pipe layers were at particular risk. The limited state of technology of the construction industry at that time meant that asbestos materials were handled with extremely high dust concentration since processing mainly used hand-held angle grinders or disc cutters. Sprayed asbestos technology also remained in widespread use and posed substantial health risks until it was banned in 1979, eight years later than in the USA. Amphibole asbestos materials were sprayed on turbines, high-rise buildings, railway wagons, on ventilation systems, and in shipbuilding.
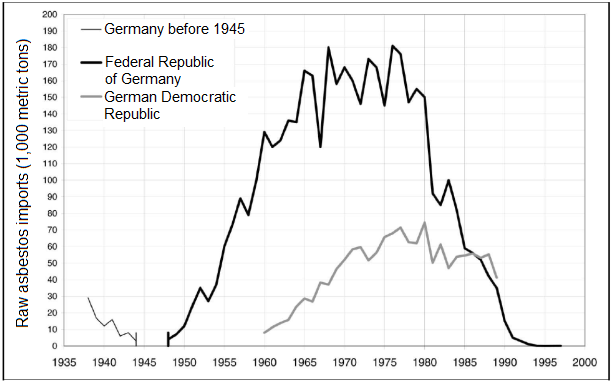
At New York at the New York Academy of Sciences meeting in 1964, Jacob and Anspach presented their research looking at asbestosis cases gleaned from a pioneering registration office for asbestos disease that had been established in Dresden in 1952.18 A total of 1512 men and 1124 women were registered there as being at risk for work-related asbestos exposure. Their jobs involved utilizing Canadian, Soviet, and South African asbestos in the manufacture of not only asbestos cement but also textiles and brake pads. Figure 1 depicts documented imports of asbestos from the 1930s, peaking in the 1960s and 1970s in both West and East Germany, and stopping in the 1990s.

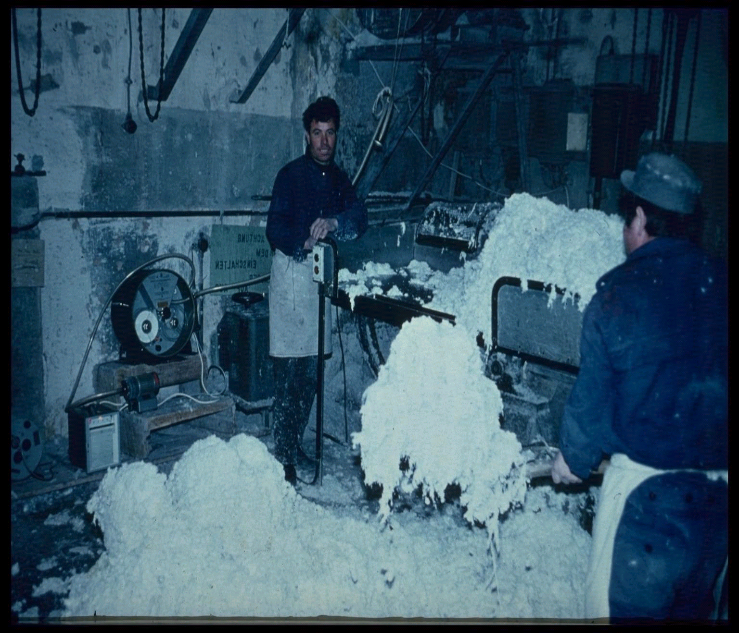
It became evident that the continued use of asbestos, predominantly chrysotile, was associated with health hazards including mesothelioma. These health hazards result from extremely high concentrations of asbestos dust for which no protective measures were in place, with no local extraction systems or cleaning facilities for dust contaminated work clothing. In the United States, the issue of keeping work and street clothes separate when dealing with hazardous materials was enshrined some decades ago. Workers mostly report that they had never been informed of the health risks they were taking when working with asbestos. Even after a century of operation, required occupational safety measures were almost completely lacking in nearly all countries.20 Examples in Figures 2 and 3 were not isolated cases.


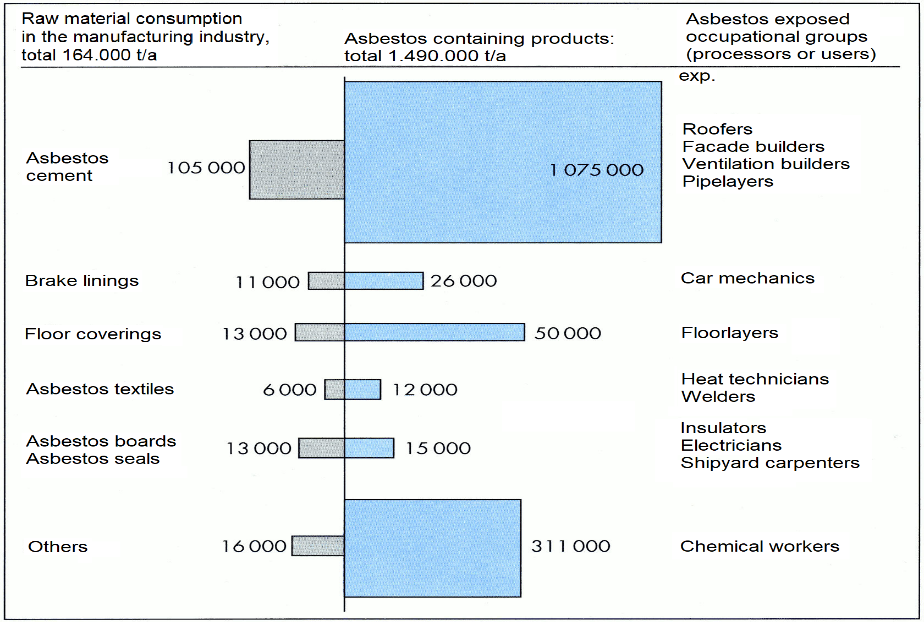
In a few workplaces, only sporadic evidence of effective measures was present including the use of personal breathing equipment to combat dust inhalation. The opposite was far more common with asbestos hazards largely uncontrolled and with no respiratory protection offered.20 Therefore, it was only reasonable to expect large numbers of chronic and fatal disease from such asbestos exposure to rise over time. In the post-World War II era, in Germany many hundreds of thousands of workers came into regular contact with asbestos cement containing chrysotile. Construction and other materials were also primarily made of chrysotile (Figure 4). Figure 4 illustrates the breakdown of annual chrysotile imports from 1975 by various industries in the Federal Republic of Germany. Estimates for the respective size of the high risk occupational groups (because of the manual work they did) were added to the chart.17

III. Findings
(i) Development and implementation of ILO’s radiological diagnostic standardization
The introductory paper on a key topic, by H. Bohlig from Luedenscheid (Germany), was entitled "Radiological Classification of Pulmonary Asbestosis."21 This was presented at the "Biological Effects of Asbestos" international conference held at the New York Academy of Sciences and organized by I.J Selikoff. As a student of E. Saupe, he had in his time gained experience with the Saupe classification of asbestosis developed in Dresden.22 Bohlig urged the International Labor Office (ILO) to draw up international agreements on a uniform radiological classification for pulmonary asbestosis. In so doing he particularly emphasized pleural calcifications and the need for their inclusion in a list of roentgenological complications of asbestosis based on his earlier observations.23,24 It should be noted that Bohlig’s demands, which were strongly endorsed by Selikoff, significantly contributed to the ILO’s chest radiograph classification initially issued in 1950.25
(ii) Early warnings
As early as 1898, Dr. H. Montague Murray, a physician at Charing Cross Hospital in London, examined a patient who was “very short of breath” and had “worked in an asbestos factory”. An autopsy was done after this patient’s death and showed that “the man’s lungs were badly scarred”. Murray considered that the workroom dust had produced the scarring in the lung.26 This patient had reported that several other young men had died earlier after relatively short periods of time working in that particular factory. In Germany, the first published case of fatal asbestosis was that of a 35-year-old female worker at an asbestos textile factory in 1914.27 In 1934, Wood and Gloyne, also in England, drawing on extensive autopsy results from two asbestos textile workers (out of a total of one hundred examined) described for the first time the co-occurrence of lung cancer and pulmonary asbestosis. The causality of this co-occurrence was later increasingly called into question by employers and their insurance institutions.28 In 1935, Gloyne communicated further findings for these two individuals both of whom had developed a squamous cell carcinoma of the lung.29 In 1936, based on another autopsy case, he reported the co-occurrence of an oat cell carcinoma with asbestosis.30 He subsequently compared the pathologic findings in silicosis and asbestosis.31 Other similar observations were being made in the United States with Lynch and Smith reporting from South Carolina in 1935 on the occurrence of lung cancer cases along with “asbestosilicosis.”32 In Connecticut in 1936, Egbert and Geiger shared the findings from the examination of an individual who had died of lung cancer together with asbestosis.33 Clearly, by 1936 at least five deaths from concomitant lung cancer and pulmonary asbestosis had been considered worth reporting in the English language literature. This was later confirmed by corresponding data in epidemiological studies.34,35 Earlier, in 1942, in his book “Occupational Tumors and Allied Diseases”, from Germany, Hueper had called asbestos a cause of lung carcinomas.36
References to the “Frequency and peculiarities of lung cancer with asbestosis” at the Dresden asbestos factory mentioned above began to occur at a relatively early stage.37 This explains why Selikoff addressed the researchers present in New York in 1964, all of them from the German Democratic Republic (East Germany), as follows: "In this regard, too, we are fortunate in having the Dresden experiences made available to us by H. Bohlig and by G. Jacob and M. Anspach, whose studies follow the classical early investigations of E. Saupe of that city".
On the international level, the 1964 International Conference on the “Biological Effects of Asbestos” held by the New York Academy of Sciences was a historic course-changing event.38 The urgent need of intensified preventive measures was shown in further human studies confirming the relationship between asbestos exposure, mesothelioma and lung cancer.39–46 A meta-analysis of 29 cohort studies encompassing 35 populations and of 15 case-control studies of asbestos exposure and laryngeal cancer undertaken by the “Committee on Asbestos of the National Academy of Science /Institute of Medicine (IOM)” provided sufficient evidence for malignancy causation.47 In the United States, the first major recognized cause of an occupational disease was high levels of exposure to silica dust in certain workplaces,48 followed by asbestos fiber dust towards the end of the 19th century in England.49
Selikoff et al. urged caution about the use of asbestos as early as 1964.1,3 No doubt this was one reason why thoughts started to turn to a follow-up conference. This conference was to be held in Dresden, in what was then East Germany, a city that had been completely destroyed in World War II. Selikoff also agreed to attend. In due course, the German “Central Institute for Occupational Medicine in Berlin” sent out invitations to the “International Conference on the Biological Effects of Asbestos”, held from April 22 to 25, 1968, under the chairmanship of E. Holstein. For us, the most important message we took from Selikoff et al. in Dresden in 1968 was that the number of deaths from asbestos-related malignancies in asbestos-exposed workers was about three times that from asbestosis.50
Baden, Schwartz, Churg and Selikoff continued to adopt a critical approach in Dresden in 1968 in their paper “Demonstration of asbestos bodies in tissue: Comparison of available techniques.”51 As had been the case in New York in 1964, the conference addressed both matters relating to lung tissue and mineral matter and the problems of pathogenesis discussed by pathologists. It was none other than G.W.H. Schepers of the Department of Health in Washington, DC, who in New York in 1964 largely confirmed Nagelschmidt’s strikingly negative results as follows: "In some of the very densely fibrotic zones, there was often less asbestos than in areas of the lungs which were less severely affected. In the pleural plaques, and in the two examples of asbestos-associated pleural mesothelioma which were analyzed, no asbestos mineral could be demonstrated."52
Selikoff made his next visit to Germany in 1975, when he attended the Colloquium of our statutory accident insurance institutions in Berlin, titled "Asbestos and Asbestosis." His presentation there was “Epidemiologic Investigations of Asbestos-exposed Workers in the United States.” Again, the most frightening of his messages for us were53:
-
About 40% of deaths among asbestos insulation workers are due to malignancy.
-
The principal hazard of exposure to the fiber is no longer asbestosis.
-
It may take much less asbestos dust to cause cancer than to result in asbestosis – “sometimes very little indeed.”
In both parts of Germany Selikoff’s message seems to have aroused disbelief at that time as the aforementioned restrictive – and by now outdated – legislation prevented such a fact from being easily ascertained.
So far, however, little attention had been paid, in Germany or elsewhere, to one particular fact: in Germany, the dangerous lung cancer risks resulting from work-related asbestos hazards were state-sanctioned from a very early date (see14).
Enterline et al. published an industry funded summary of findings in the United States in 1978.54 Like other studies, Enterline et al. did not address the minimum dose if any required to cause lung cancer. Case reports have documented that exposures of as little as one day have caused mesothelioma.55,56 This has been shown in animal studies as well.57,58
In German-speaking countries, in spite of a publication on the aforementioned first case of severe asbestosis in 1914,27 this causal relationship was not widely discussed prior to the 1930s. In 1938, Hornig59 and Koelsch60 drew attention to asbestos-related lung cancers. Nordmann, investigating the still relatively low number of fatalities from asbestosis, found a 17% occurrence of lung cancer among such individuals.61 Furthermore, Wedler, on the basis of similar individual case studies, expressed the view that asbestos caused lung cancer.62 In Austria, Teleky noted that he thought asbestosis was responsible for the development of lung cancers.63 A 1941 experiment involving mice, Nordmann and Sorge, showed that inhaled asbestos dust caused lung cancer in animals.64
In 1940 in Berlin, Kühn undertook a detailed analysis of dust in the lungs of patients with asbestosis, making use of a newly developed Siemens’ electron microscope for the first time.65 However, at that time he could not detect chrysotile fibers within the asbestos bodies with this EM device. He could only detect amphibole fibers inside asbestos bodies. In 1941 Kühn confirmed early lung fiber and asbestos body investigations by the Swedish mineralogists Sundius and Bygden.66 In 1943, Wedler discovered that asbestos caused mesothelioma and separated this tumor from asbestos-related lung cancer.67,68
(iii) German regulations on reducing asbestos exposure in the workplace
Almost one hundred years after the first industrial uses of asbestos, in 1969, long term efforts finally succeeded in establishing occupational health examinations of workers employed in settings where asbestos was used.69,70 These national regulations specifically required that occupational safety and health procedures coming into force in 1973.71 This included requirements to limit asbestos exposure in workplaces. From 1976 onward these threshold limits were lowered step by step until after long resistance, the national ban on asbestos was reached in 1993 (Table 1).8 This was associated with a significant decline in asbestos workplace concentrations.72 However, there was no evaluation of health-related effects of these regulations on workplace exposures.
(iv) History of legal definitions of asbestos-related diseases
In 1884, statutory accident insurance institutions (i.e., branch-orientated employers’ liability insurance associations, financed by employers exclusively) were established in Germany. Initially their responsibilities had been confined to occupational accidents only. Their obligations were expanded in 1927, meaning that they also had to pay appropriate compensation in case of occupational diseases. This expansion was mainly due to the sharp increase in fatal dust-related lung diseases during the Industrial Revolution at the end of the 19th century. Asbestosis was the first ARD included 1936 in the list of occupational diseases74 and in 1942, in the middle of World War II, lung cancer caused by asbestos inhalation followed.75 (Table 2).
In his book “The Nazi War on Cancer,” Robert N. Proctor14 acknowledged that German physicians had already documented the health hazards of asbestos in the 1930s. As he noted, asbestosis was included in the list of occupational diseases in 1936 and in 1942 Germany became the first nation to recognize lung cancer caused by asbestos inhalation as a compensable occupational disease. By that time a wide range of public health measures were passed including, among others, aggressive antismoking campaigns, restrictions on asbestos use, as well as radiation, pesticides, and food dyes. Nazi health officials introduced strict occupational health and safety standards. However, the perverted Nazi ideologies intended to protect only those of the “nordic race” from these hazards.
Until 1997 lung cancer acknowledgement and compensation was subject to an extremely effective restrictive practice: the tumor diagnosis always had to be accompanied by additional proof of asbestosis such as frequent diagnoses by insurance-affiliated pathologists (details on this are given in the section (vii below).76 Consequently, H. Bohlig et al. could only cite 40 cases of asbestos-related lung cancer that were published or recorded by the employers’ statutory accident insurance institutions from 1938 to 1959.77 Indeed, at that time, there was no way for those on the relevant medical advisory board of the Federal Ministry of Labor to remove this from the existing regulations, i.e., the requirement for asbestosis to be proven in order for a case of asbestos-induced lung cancer to be recognized as such. Once again, the very valuable assistance provided by Selikoff and his staff was vital, helpful, and necessary for Germans to finally overcome this obstacle in 1992 by recognition of the 25 fiber-year dose as the legal alternative prerequisite of lung cancer (Table 3).78
In the 1990s, in addition to clinically and radiologically defined asbestosis or pleural disorders, the latter associated with lung cancer or laryngeal cancer in combination with asbestosis of grade 1 or higher, or pleural disorders due to asbestos, or an asbestos dose of at least 25 fiber-years became occupationally recognized diseases in Germany (Table 3).79–81 The same is true for lung cancer caused by the interaction of asbestos dust and polycyclic aromatic hydrocarbons, by evidence of exposure to a cumulative dose which equates to a probability of causation of at least 50 per cent. In 2017, the inclusion of cancer of the ovary followed, based upon a meta-analysis which identified nearly a doubling risk causation in asbestos-exposed females (Table 3).82 The stepwise implementation and extensions of prevailing German legal definitions of asbestos-related occupational diseases and their occupational disease numbers are shown in Table 2 with its current definitions in Table 3.
According to paragraph 9, section 2 of the German Social Law VII (Sozialgesetzbuch VII83) beyond the legally binding list of currently 84 occupational diseases,84 in principle a disease can also be acknowledged and compensated if new scientific evidence clearly documents an occupational cause of such diseases, and the other legal preconditions of an occupational disease are fulfilled. However, due to its very high bar (among others, a doubling risk of a disease due to a defined occupational exposure proven in an occupational group by epidemiological studies is required), this opening of the occupational diseases list has rarely been applied.
Because more limited evidence exists for asbestos causation of colorectal cancer, cancers of the stomach85 and oropharynx,46,47 these disorders have not been included in the list of occupational diseases and have not been acknowledged and compensated.
The European Union has not agreed upon a legally binding list of occupational diseases. However, there is a list of recommended diseases to be acknowledged as occupational diseases.87 This list includes all of the asbestos-related diseases that have been in force in Germany with minor modifications in most European countries. Exceptions in other countries are the exclusion of asbestos-related pleural abnormalities as an occupational disease in the European list and the dose of 25 fiber-years for acceptance of lung cancer applied in Germany. However, there is medical support for such a specific threshold dose and recent publications indicate a dose of 4 to 5 asbestos fiber years for doubling the risk of lung cancer.88–90
(v) German guidelines on diagnostics and compensation of asbestos-related diseases
The first version of guidelines on diagnostics and compensation for asbestos-related diseases was issued in 2011 on the basis of a consensus of concerned national medical societies and institutions.91 These came after decades without such operating guidelines and great variations in diagnostic procedures and interpretations. These guidelines were updated in 2020.92 They are not legally binding, but they are based on expert knowledge, existing literature and operating experience and include algorithms with a step wise approach to the diagnosis of asbestosis, asbestos-related pleural disease including pleural fibrosis, and the malignancies noted in Table 3. Histopathologic confirmation is needed for suspected asbestos-related malignancies and for the resolution of differential diagnoses but is not recommended for the diagnosis of non-malignant asbestos-related disorders. The diagnosis is always based upon a detailed exposure assessment, an occupational history, a medical history, an analysis of latency, clinical findings, radiologic changes and lung function. The occupational history, lung function testing and chest X-ray are the basic main elements needed to identify non-malignant asbestos-related disease. Since chest X-rays are limited in their sensitivity and specificity, high resolution computerized tomography is recommended in the initial diagnosis of all suspected asbestos-related disease, and is especially needed in cases with questionable x-ray findings.93 The degree of compensation for occupational diseases depends on the details given in tables 6 through 9 of the guidelines noted above for the diagnosis and compensation of such diseases.91,92
(vi) Official numbers for asbestos-related diseases in Germany
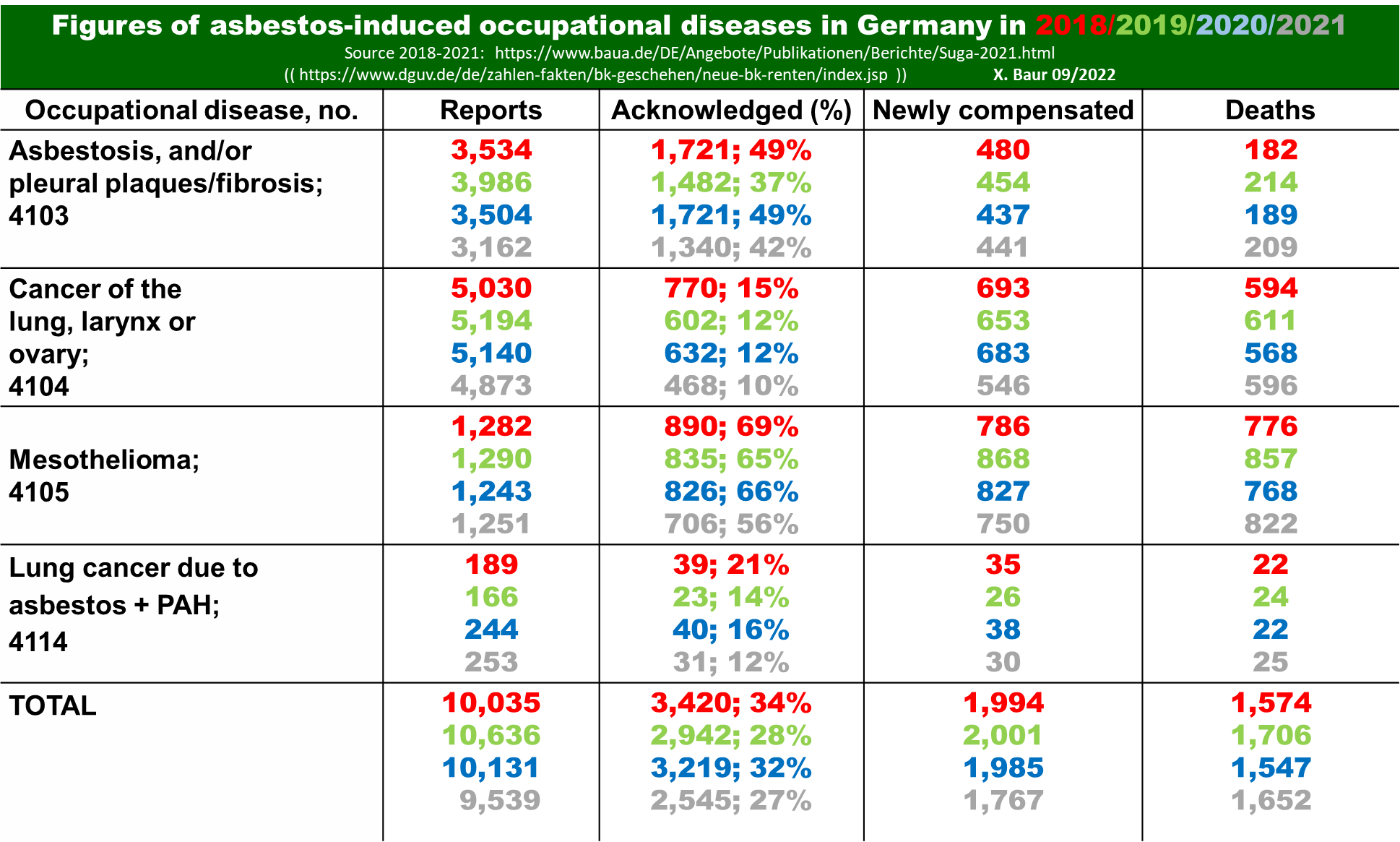
Since asbestos-related malignant diseases have a mean latency of about forty years, there has recently been a large increase of slightly lower reported latency numbers. During the period from 2018 to 2021, the numbers of asbestos-related diseases reported annually have been in the range of 10,000 of which about 3,000 have been noted officially to be occupational. About 2,000 have been compensated, while about 1,600 have died. Interestingly and not rationally, the rate of accepted and compensated cases has been declining for all ARDs. There is evidence that asbestos-related lung cancer is significantly underreported for a variety of reasons. In Germany about 60% of mesothelioma claims are accepted as an occupational disease. For lung cancer the rates for acknowledgement and compensation are much lower, in the range of 10-15% (See Table 4). For all ARDs the mean duration of exposure to asbestos was eighteen to twenty years and the mean age of death is sixty-seven. Asbestos-related diseases comprise about 65% of all deaths due to occupational diseases.11,19
As mentioned, about 95% of imported asbestos has been chrysotile; however, some workers also likely had occupational exposure to amphiboles. There was detailed documentation of 67 mesothelioma cases who were exposed to Russian chrysotile only, which was reported – but never proven – to be free of amphiboles.19

(vii) Development and implementation of unsound restrictive asbestos-based diagnostic criteria
In 1927, Germany extended the legal liability for statutory accident insurance institutions by including prevention by "all appropriate means" for compensable diseases and required the rehabilitation of occupational diseases (Bundessozialgesetz VII83 – this meant that the direct responsibility of the individual employer for compensation of occupational accidents and diseases disappeared because it was transferred to these accident insurance institutions).
Instead, the employers’ liability statutory accident insurance institutions took on the responsibility of paying for the consequences of recognized occupational diseases, in addition to their already existing responsibility for the consequences of work-related accidents. As a result, as opposed to other countries, such as Italy (see e.g., currently ongoing trials accusing previous asbestos plants’ owner Schmidheiny of being responsible for the death of many of his asbestos workers), even in illegally extreme health endangering working conditions, no employer has been brought on trial so far.
On the international level, the asbestos industry and their insurance systems blocked publications of early observed asbestos-related adverse health effects, manipulated science and public opinion and inhibited restrictive regulation of asbestos.48,95–98 The asbestos industry also mounted public relations campaigns99,100 with the aid of its employees and associated vested scientists.101 The idea was to counter the negative publicity surrounding asbestos given the increasing reports of lung cancer and malignant mesothelioma cases.102 One of the most prominent such scientists in Western Germany at the time was Professor Herbert Otto of the University of Erlangen’s Institute of Pathology.
By the middle of the 1960s, Otto had predicted there would be a sharp increase in the number of asbestos-related diseases after 1968. He had considered Zenker’s historic lung dust analysis (for details see chapter 2 of the Appendix with Figures 1a, b) and his own studies regarding silicosis.103 He concluded that the severity of asbestosis would depend upon the quantity of dust deposited in the lung and he then developed a hypothesis that a concentration of at least 1,000 asbestos bodies per gram wet lung tissue represented a prerequisite for the diagnosis of asbestosis Grade 1, a so-called minimal asbestosis.104 To this end he developed a method of asbestos body quantification in ashed lung tissue making use of light microscopy.105 This methodology for some time has been scientifically discredited as not sensitive and specific enough as such analysis ideally should require proper TEM study.106–112
There is a legitimate issue in characterizing what should be considered asbestosis grade 1 but was considered a fixed thesis put forward by Otto at a pulmonary conference in Freudenstadt in June 1965.113 Otto was afraid that workers would inadequately claim compensation for an occupational disease. In particular he referred to asbestos-related lung cancer figures and that the accident insurance institutions would suffer if compensation requirements were not made more restrictive. He proposed requiring lung dust analysis and the measurement of asbestos bodies in lung tissue as a diagnostic tool. Otto, who had early in his career forged ties with the insurance industry, made use of this unsound scientific view of asbestos body counts (and rarely of asbestos fiber counts) in diagnosing asbestos-related lung conditions.103,114–117 Otto’s critical but unsound comments – which he expressed when he was an unsalaried lecturer – eventually came to the attention of the German statutory accident insurance institutions (Berufsgenossenschaften).113,118–121
From the insurer’s perspective it made sense to use these new restrictive diagnostic criteria.121 If these restrictive standards were to be applied nationwide, and potentially in settings beyond Germany, the required lung testing in his institute would become an important diagnostic procedure and would save insurance industry funds.104,105,122–125 Otto then became the leading medical authority for the employers’ statutory accident insurance institutions of West Germany.
The definition of at least Grade 1 asbestosis was one of the alternate preconditions required for compensation of asbestos-related lung cancer (see Table 2). The diagnosis of Grade 1 asbestosis has been a prerequisite for acknowledgement and compensation of asbestos-related lung cancer in the absence of asbestos-related pleural changes or an exposure of at least twenty-five fiber years; i.e., use of the 1,000 asbestos body standard as a precondition in these cases that would be difficult to meet. This became the working practice as early as 1965.
Consequently, the quantification of asbestos bodies in lung tissue was increasingly used as a criterion to limit compensation for asbestos-related lung cancer. It was not only applied to lung cancer, but also in pathology diagnostic interpretation of lung fibrosis of asbestos workers. As a result, many cases of asbestosis have been misdiagnosed as idiopathic pulmonary fibrosis.126–128
Regardless of the occupational history of asbestos exposure or the location of fibers in pleural tissue which was usually not investigated, Otto claimed that nearly one-third of mesothelioma cases in Germany were not related to prior occupational exposures to asbestos. Financed by employers’ statutory accident insurance institutions, he presented his own data on the issue.129 He concluded that nine of the thirteen mesotheliomas he studied were wholly "spontaneous." He reported that there was only low-grade asbestosis in these subjects. He therefore opined that lung dust analyses should be undertaken in every mesothelioma autopsy. (for more details see chapters 2 and 3 of the Appendix).
As noted above, brief exposures can cause mesothelioma but not result in elevated lung asbestos levels. Thus, application of high fiber count requirements would misclassify these cases as “spontaneous” and unrelated to asbestos exposure.
The statutory accident insurance institutions followed Otto’s proposal rather than legislative requirements that were in place, adopting the criteria of 1,000 asbestos bodies per cc of lung tissue as a criteria for compensation.125,130 German insurance companies also adopted a count of 50 asbestos bodies per cc as a requirement for occupational exposure acknowledgement and compensation of mesothelioma. In lung cancer cases they required at least Grade 1 asbestosis with a minimum of 1,000 asbestos bodies per cc of lung tissue.131 Thus compensation for lung cancer required a twenty-fold higher asbestos count than that required for mesothelioma.
The Federation of the statutory accident insurance institutions repeatedly informed nationwide pathologists and clinicians that autopsied lungs or lung specimens for subjects thought to suffer from asbestos-related disease were to be sent to their Mesothelioma Register headed by Otto. In that setting an additional examination would be carried out to determine the quantity of asbestos deposited in the lungs.111,112 By doing so lung tissues have been analyzed on behalf of the statutory accident insurance institutions in about one thousand cases annually and those findings were applied in their decisions on accepting or declining claims for acknowledgement and compensation of asbestos-related diseases, especially lung cancers.
Otto had ignored all contradictory findings, and this was similarly the view adopted by his successors and the insurance industry. Despite overwhelming scientific evidence that this approach is inappropriate, Otto’s successors have continued to recommend measuring fiber counts in lung tissue for the assessment of asbestos exposure, including the measurement of all type of fibers.105,132 Although their data has been found to be misleading by many others,94,126,127,133 they continue to believe that 400 asbestos bodies per cc of wet tissue is required to demark asbestosis from idiopathic pulmonary fibrosis or lung fibrosis due to other inhaled noxae such as silica and metal dust.105,132
Similarly, Roggli from the US has proposed inappropriate diagnostic criteria.134 In recent years, Roggli has testified primarily for companies and his interpretation of what is considered asbestosis has been modified.135,136 Woitowitz and others have tried to counter these unsound decision-making pathology diagnostic criteria and to give judges a better understanding of the differences between amphiboles and chrysotile fibers as found in the human lung, and how that is also different from the findings associated with silica exposure.137
(viii) International spread of restrictive asbestos-based compensation practices
Others have proposed similar restrictive criteria. For example, Roggli applied fiber count criteria as a basis for denying asbestos as a cause of mesothelioma among car mechanics exposed to chrysotile from brake pad dust.134,138–143 Spain also has adopted fiber count criteria.144,145 Switzerland, where there had been a considerable global asbestos cement industry, argued in 1975 that asbestosis should not be confirmed until asbestos was detected in lung tissues.146 This has been further commented upon by Woitowitz.111,112
The Canadian chrysotile industry with its International Chrysotile Association as a lobby group, called the Asbestos International Association (AIA), propagated Otto’s asbestos body diagnostic criteria in the United States and Canada. Dr. P. V. Pelnar, a medical consultant and scientific secretary and member of the Institute of Occupational and Environmental Health and the Canadian chrysotile industry in Montreal, promoted Otto’s views. This included stating that there existed spontaneous mesotheliomas not caused by asbestos and required a coexistence of asbestosis to causally link occupational exposures to the development of mesothelioma.
As mentioned in detail in the section Concluding Remarks below, at the asbestos Helsinki conferences in 1997 and 2011, Roggli as chair of the pathology area group was able to put forward his restrictive fiber-based diagnostic criteria for asbestosis and asbestos-related lung cancer.147,148 His service as a defense expert in more than a thousand cases only became public later.
(ix) Consequences
At the 1975 Berlin Asbestos Colloquium entitled “Asbestosis Problems From a Morphological and Dust Analysis Perspective”, corporate representatives in the audience found Otto’s hypothesis extremely promising.149 This hypothesis would eventually be highly successful not only for Germany’s employers’ liability insurance and the statutory accident insurance institutions, but also, among others, for the Canadian chrysotile industry. Otto asserted that only if “enough asbestos bodies” are detected can a reliable diagnosis of occupational asbestos exposure be made. Thus, patients with interstitial fibrosis due to asbestos could only be diagnosed with a sufficiently high number of asbestos bodies, something that would be unlikely to occur following exposure to chrysotile asbestos and might not be met several decades after last exposure for any forms of asbestos.4,111
Since the asbestos body requirements reduced the number of compensable cases, the asbestos industry and insurance institutions began to promote and apply the compensation criteria in Germany.125,130,150 With its adoption, the criteria which were initially adopted for the diagnosis of “minimal asbestosis” soon served as the basis for rejection of asbestos-induced lung cancer and other asbestos-related diseases. This was especially complicated by the restrictive histologic definition of asbestosis by Roggli et al.134 which transferred early abnormalities classified previously as asbestosis Grade 1135,136 to asbestosis Grade 0.136 These criteria have resulted in the rejection of 85 % to 90% of reported asbestos worker’s lung cancers as an occupational disease. Table 4 shows the most recent official statistics for 2021; it reveals that only 10 % of 4,873 claims of asbestos-related cancer in German were accepted as asbestos related.
(x) Criticism of the asbestos body hypothesis and the related compensation practice
Otto disregarded serious scientific objections to his theory, especially that following chrysotile exposure it was unusual to detect fibers and asbestos bodies in human lung decades after exposure. It also was not commented upon by Otto that chrysotile fibers would move more easily to the pleura than amphiboles. Otto ignored Drs. Sundius and Bygden and others who had identified chrysotile asbestos as the main cause of asbestosis as early as 1938.66 They had noted early that “the lung is apparently able to break down chrysotile asbestos fibers” and did not generate asbestos bodies and would not be counted post mortem or in biopsies. In 1965, Nagelschmidt noted coal and silica dust can be easily found in the lung but asbestos fibers diminish over time.151 He cited Beattie and Knox in 1961 who found that chrysotile exhibits a short half-life in the lungs of patients with asbestosis.152 Nagelschmidt wrote “there is no clear correlation between the average lung dust concentration and the grade of asbestosis, but the lungs with the highest grade of fibrosis had the lowest calculated dust accumulation rates… no positive identification of chrysotile could be made in a human lung with asbestosis in any published work to date”.100 Nagelschmidt was critical of Otto’s results and stated that no asbestos was found in over half the lungs with asbestosis that Nagelschmidt examined. He noted “the most likely explanation is that asbestos gets dissolved in the lungs. The process of dissolution is likely to start with the removal of the cations, magnesium, sodium, iron, and aluminum which would leave a skeleton of hydrated silica of polycyclic acid”. Nagelschmidt also noted that "similar views with regard to the action of chrysotile had already been expressed by Berger". He was referring to the work of P.J. Berger.153,154 Indeed, Otto admitted as early as 1965 that "these [Nagelschmidt’s] findings could support the repeatedly expressed claim that asbestos needles dissolve in the lung and thus disappear".
In 1965, Selikoff et al. published a paper on asbestos lung fiber analysis.155 They noted that “the demonstration and localization of asbestos fibers in tissue has been and remains essential for the study of pathogenesis of asbestosis and its complications and for the investigation of the biological effect of the fibers on a cellular level.” However, they acknowledge that fibers that “…generally, asbestos bodies are only visible some time after the initial inhalation”. Selikoff continued with the following warning “Leicher sought asbestos bodies in a mesothelioma but found none, nevertheless he was able to demonstrate fibers by X-ray techniques applied to tumor tissue” and “Nagelschmidt was unable to find asbestos in ashed mineral in a case of severe asbestosis.”156
Supporting this refutation is the work of Elmes and Wade published under the title “Relationship Between Exposure to Asbestos and Pleural Malignancies in Belfast*.”*157 At the time they presented, their counts of asbestos bodies in lung tissue for no fewer than 200 deaths from non-malignant disease as well as 100 other males who had died of lung cancer and 42 from mesothelioma showed that “in carefully matched control groups the incidence of asbestos exposure and of asbestos body in the lung is only 1 in 4.” Even with asbestos disease these may be few fibers or asbestos bodies found. They went on to write that "the methods of detecting both previous exposure to asbestos and the presence of asbestos in the lungs used in the study are not very efficient, and our data indicate that in both instances about one quarter of the patients were incorrectly recorded as negative." In conclusion they wrote “among asbestos workers carcinoma of the lung is at least as important as the more specific mesothelial tumor of pleura or peritoneum”.
At the 1964 conference with 1,100 attendees (published in the Ann NY Acad Sci in 1965), Hourihane of the London Hospital Medical School and others also criticized the asbestos body diagnostic criteria.158 Hourihane noted that asbestos bodies could not be identified in the majority of biopsy material and sputum samples from 74 patients with mesothelioma who had a history of asbestos exposure. He reported that "asbestos fibers are found within the mesotheliomatous tissue in about one quarter of the cases, and in about one half of the cases if only patients with asbestosis are considered." By 1975 at the Berlin Colloquium Otto continued to promote his asbestos body hypothesis and he neglected to adequately mention any contradictory results in the literature.151,159
German experts recognized the difficulty of findings these bodies when some at the Dust Research Institute of the German Federation of Statutory Accident Insurance Institutions reported that when they used electron microscopy to analyze dust samples from seventeen lungs with asbestosis provided by Otto, no chrysotile was detected although it was clearly the predominant fiber used in German industries.160 As has been suggested by others, and as would be expected with a good occupational history, exposure to chrysotile should generally be assumed in such diseased cases. These findings at the Dust Research Institute was found to be consistent with the work of Nagelschmidt.
Dr. Jacob Churg, a professor of pathology at the Mount Sinai School of Medicine in New York, who worked closely with Selikoff on issues of asbestos wrote106–110:
“…my feeling and that of Dr. I.J. Selikoff and Dr. Langer is the same as yours. The conditions that there should be a ‘more than normal’ amount of asbestos by light microscopy in the lungs of patients who have cancer or mesothelioma and who give a history of exposure to asbestos, is much too restrictive. I quite agree with you that chrysotile asbestos is not only removed via lymphatics and via bronchi but also disintegrates in the lungs, so that thirty years later when malignancy appears, the amount of asbestos in the lung may be very small. Furthermore, light microscopic examination is not the best procedure to measure the number of fibers and bodies; electro-microscopy is much to be preferred. Dr. Langer and Dr. I.J. Selikoff have written a paper on chrysotile asbestos in the lungs of persons in New York City (Langer, Selikoff, Sastre Archives Environmental Health 22:348-361, 1971). In the United States, according to Dr. I.J. Selikoff the only precondition for compensation from mesothelioma or lung cancer is a history of exposure to asbestos”.
Over the years many others have found Otto’s diagnostic criteria to be problematic. This includes the work of Dodson161–163 and Pezerat.164 Others have commented on the fallacy of Otto’s assumptions including work from animal experiments, epidemiological studies,126 and others which have discussed the importance of the occupational history combined with lung dust analysis.165 Pezerat proposed a “hit and run phenomena”.137 He hypothesized that inhaled chrysotile fibers could produce genotoxic effects on target cells but be undetectable decades later, especially if one only uses light microscopy.164
None of the aforementioned discussion over time has persuaded either Otto or his successors.105 Their management of the German Mesothelioma register has led to them to deny this theory and the fundamental differences of serpentine and amphibole asbestos in the lungs and in the pleura. They have remained unmoved in their views even after these counterarguments have been proposed and successive judgments in German national social state courts quotes have ruled against use of their documentation. Otto and his successors have succeeded in erecting a high bar to the recognition of many occupational diseases resulting from exposure to asbestos. On an international scale Roggli who has been part of the Helsinki Criteria Document Panels has put forth similar arguments as outlined in the following section.
Many in the scientific community have responded to this continued inappropriate point of view including the Collegium Ramazzini166 and Baur et al.12,94,167 (see also chapters 5 and 6 of the Appendix).
All of the aforementioned findings support the significant notion, which is supported in the Helsinki Criteria documents (with some divergent statements in its pathology part mentioned above), that one needs a sophisticated occupational history which truly gives a more accurate picture of an individual’s prior exposure. It should also be noted that there is, at this time, no generally accepted laboratory methodology for analysis of fibers or asbestos bodies in tissue, and that each laboratory which does this type of work is expected to have its own set of criteria and laboratory specific values.148 This further adds to the unreliability of any notion of doing tissue digestion or asbestos body or fiber counts and making them comparable in different settings.
As noted earlier, the applied restrictive diagnostic criteria are wrong is especially evident in the ratio of rejected cases of asbestos-induced lung cancer. Also speaking to this issue is the much more widely noted ratio of asbestos-induced lung cancers to mesotheliomas, which is not the same ratio that would be recognized in the German compensation system. This includes the work of Selikoff et al.50 and others including that of McDonald.9,168,169 Even a small German study confirms this ratio of more lung cancers than mesotheliomas being caused by asbestos.170
IV. Concluding remarks
Increasingly it has been noted that there are considerable costs for the treatment, rehabilitation, and early retirement arising from asbestos-induced occupational diseases. This is especially true for fatalities.5,171,172 Because of the continued adoption of the aforementioned restrictive diagnostic criteria, costs that should be borne by the asbestos industry and their insurance systems in Germany by the statutory accident insurance institutions are shifted to other health benefits and pension insurance schemes which should not be primarily responsible for such costs, respectively.95 Since 2012 more than 2000 lung dust analyses using light, but rarely electron microscopy, had been carried out annually to present to the statutory accident insurance institutions as a basis for claim denial.173,174
In Germany, compensation for asbestosis started as early as 1936 followed by compensation for asbestos-related lung cancer, pleural disorders, mesothelioma, laryngeal and ovarian cancer, as well as lung cancer caused by exposure to asbestos plus polycyclic aromatic amines (see Table 3). The diagnosis made by the usual diagnostic criteria used by clinicians has always been based on an occupational history documenting an asbestos exposure together with histopathologic findings in cases of malignancy. With the exceptions of acknowledgement of asbestos-related pleural abnormalities and of asbestosis Grade 1 as a precondition for asbestos-related lung cancer to be an occupational disease, German criteria are similar to the European Union listof recommended asbestos-related occupational disease criteria.87
The extremely restrictive diagnosis based on asbestos body and fiber counts has made things more difficult for injured workers. It especially ignores that chrysotile undergoes translocation, clearance and degradation much more easily in the lungs than amphiboles and is far less likely to create asbestos bodies164,175–180; and chrysotile represents the majority of asbestos used in Germany and around the world. Roggli, who is noted to be a witness these days primarily against workers in asbestos litigation, has been aware of the German restrictive diagnostic criteria and has denied that friction from chrysotile-based brake pads causes mesothelioma.181 Roggli has gone on to put forth similar restrictive diagnostic requirements in the United States and introduced them within the Helsinki documents.182 He has even gone so far as to recharacterize asbestosis Grade 1 into asbestosis Grade 0.134,136
These unsound restrictive pathology practices have resulted in declining many thousands of compensation claims of asbestos victims with significant financial savings for the manufacturers and users, particularly users of chrysotile asbestos.111,112,134,138–146 In recent years in Germany only 468 to 770 asbestos-related lung cancers per year were accepted although there were about 5,000 cases reported annually. These activities raise issues, not only relevant to Germany and other countries, but also relevant to the continuing widespread use of asbestos in some parts of the world and future compensation in many countries.
An outcome suggested by this paper is the need of to broaden the WHO beneficial initiative to eliminate ARD worldwide by establishment of an international board of independent scientists to work on remedial action on an international scale that would develop acknowledgement and compensation criteria that follow the science. This will shift the economic burden onto the industry that caused the diseases rather than socializing the costs while privatizing its profits. Such a board could be supported by national legal branches recognizing possible regional deviations and initiating compliance with the recommendations.
For further detailed information see the following Appendix